P5046 - Dupilumab in the Treatment of Persistent Eosinophilic Esophagitis Causing Refractory Anastomotic Stricture After Ivor Lewis Esophagectomy for Esophageal Adenocarcinoma
Nova Southeastern University College Of Osteopathic Medicine Davie, FL
Michael Thomas. Hsieh, BS1, Chelsea B. Ramos, 2, Nabiha Atiquzzaman, BS3, Harinath Sheela, MD4, Srinivas Seela, MD5, Moin Kola, MD4, Seth Lipka, MD4 1University of Central Florida College of Medicine, San Ramon, CA; 2University of Central Florida, Orlando, FL; 3Nova Southeastern University College Of Osteopathic Medicine, Davie, FL; 4Digestive and Liver Center of Florida, Orlando, FL; 5Digestive and Liver Center of Florida, LLC, Orlando, FL Introduction: Anastomotic strictures are a common postoperative complication of Ivor Lewis Esophagectomy, most often caused by acid reflux or ischemia. However, anastomotic stricture caused by eosinophilic esophagitis (EoE) is exceedingly rare, particularly in the postoperative setting. Here, we present a case of adenocarcinoma arising in a patient with long-standing EoE, and who developed PPI- and steroid-refractory anastomotic stricture years after esophagectomy.
Case Description/
Methods: This 45 year old male patient with no significant past medical history underwent routine endoscopy for GERD and dysphagia demonstrating 15 eos/hpf confirming EoE (2016). Patient was doing well on twice a day PPI and had repeat endoscopy for GERD symptoms without significant findings. In 2017, repeat endoscopy showed GERD features. In 2018, patient was experiencing dysphagia and subsequent endoscopy revealed a nodule in the distal esophagus with adenocarcinoma as well as persistent mid-esophageal eosinophilia (20 eos/hpf). Staging confirmed T2N0 tumor without metastasis. The patient underwent Ivor-Lewis esophagogastrectomy in 2019, and no recurrence was detected through 2020.
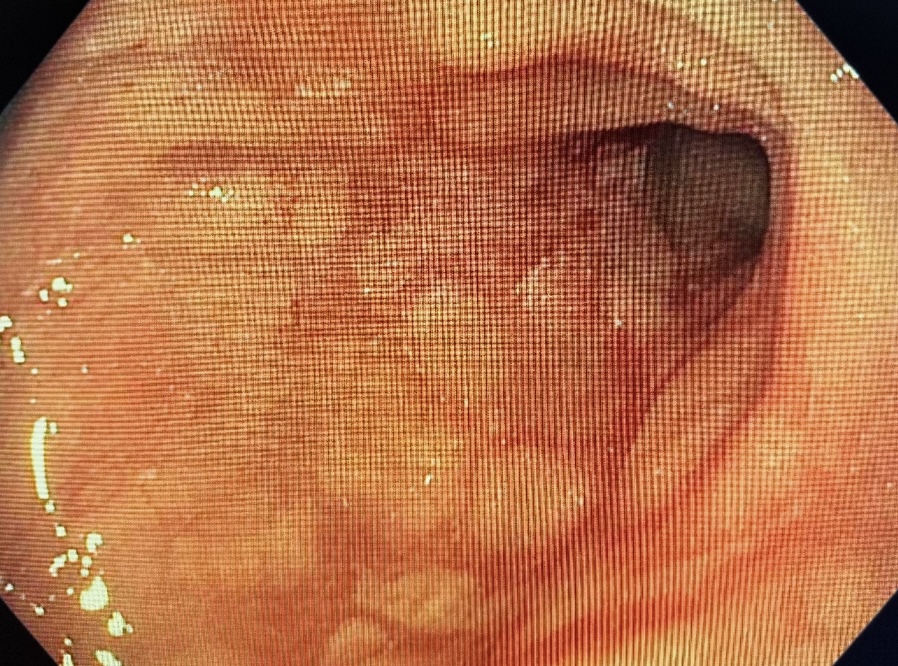
Patient developed significant dysphagia in 2022 requiring TTS dilation for 10mm stricture dilated up to 13.5 mm. Despite PPI twice a day, follow up endoscopy in 2023 revealed 71 eos/hpf and subepithelial fibrosis, requiring dilation to 15 mm with TTS balloon.
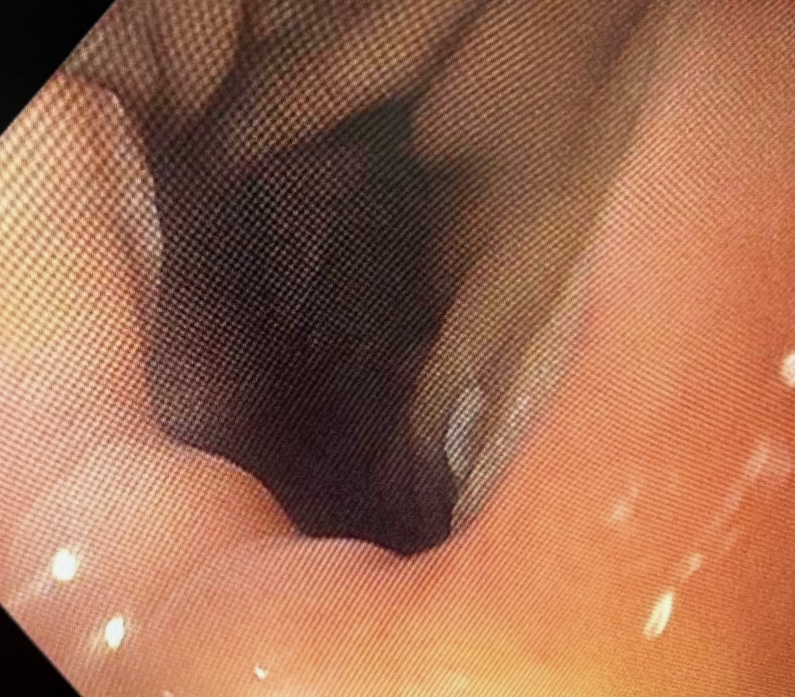
Patient had follow up endoscopy requiring dilation to 15 mm and was placed on budenoside in 2024 (30 eos/hpf). However, symptoms recurred several months later requiring repeat dilation with a Savary dilator to 15 mm (50 eos/hpf) and was placed on dupilumab with follow up endoscopy without eosinophils 2 months later. Patient has been asymptomatic on dupilumab 6 months post treatment.
Discussion: This case highlights a rare etiology of anastomotic stricture induced by EoE. In patients with resistant stricture refractory to twice a day PPI or topic steroids, biologic therapy with dupilumab may offer benefit in cases of EoE-associated anastomotic stricture.
Figure: Image 2: Resolution of anastomotic stricture following dupilumab therapy (2025)
Disclosures: Michael Hsieh indicated no relevant financial relationships. Chelsea Ramos indicated no relevant financial relationships. Nabiha Atiquzzaman indicated no relevant financial relationships. Harinath Sheela indicated no relevant financial relationships. Srinivas Seela indicated no relevant financial relationships. Moin Kola indicated no relevant financial relationships. Seth Lipka indicated no relevant financial relationships.
Michael Thomas. Hsieh, BS1, Chelsea B. Ramos, 2, Nabiha Atiquzzaman, BS3, Harinath Sheela, MD4, Srinivas Seela, MD5, Moin Kola, MD4, Seth Lipka, MD4. P5046 - Dupilumab in the Treatment of Persistent Eosinophilic Esophagitis Causing Refractory Anastomotic Stricture After Ivor Lewis Esophagectomy for Esophageal Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.