Icahn School of Medicine at Mount Sinai New York, NY
Isha Bhutada, MD1, Samuel Acquah, MD2, Serre-Yu Wong, MD, PhD1 1Icahn School of Medicine at Mount Sinai, New York, NY; 2Mount Sinai Health system., New York, NY Introduction: Multiple myeloma (MM) is a bone marrow-based plasma cell neoplasm. Extramedullary involvement is a relatively uncommon complication, with current descriptions of gastric metastasis in literature primarily limited to case reports. Overt GI bleeding from malignancy, which has been found to be responsible for only 1 to 5% of UGIB, can present similarly to and concurrently with more common etiologies such as mucosal injury. Recognizing hematologic malignancy as a potential contributor—especially in the setting of endoscopically visible lesions—is critical for prompt diagnosis and management.
Case Description/
Methods: A 71-year-old male with a known history of MM presented with new left leg swelling. Initial vital signs were notable for a BP 108/76 and HR of 109 bpm. Labs were significant for leukocytosis (WBC 16.7 x 109/L), anemia (Hgb 9.8 g/dL; baseline 10.5) and BUN 58 mg/dL. Physical exam showed 3+ LLE edema. Duplex ultrasound ruled out DVT. CT A/P revealed a 7.5cm left thigh mass consistent with plasmacytoma and incidental nodular soft tissue thickening in the epigastrium and omentum, concerning for extramedullary spread.
On hospital day 3, VDCEP chemotherapy and high-dose dexamethasone were initiated. He then developed multiple episodes of melena and was started on IV Pantoprazole. Hgb dropped to 6.9 g/dL, requiring 1u pRBC, with subsequent under-correction requiring additional transfusion. EGD revealed LA Grade D esophagitis (non-bleeding), erythematous gastric mucosa with numerous nodules, and duodenal ulcers (non-bleeding). Biopsies of the nodules confirmed plasma cell infiltration, genotypically consistent with known MM.
GI bleeding was attributed to steroid-related mucosal injury, though contribution from the malignant gastric infiltration could not be excluded. The patient remained hemodynamically stable despite intermittent melena. He continued systemic treatment with VDCEP. Discussion: This case illustrates a rare but important GI manifestation of multiple myeloma: gastric plasma cell infiltration, possibly presenting with upper GI bleeding. While GI bleeding can be a complication of cancer due to coagulopathy and therapy-induced mucosal injury, providers should also consider tumor infiltration in patients with known hematologic malignancy. Gastric involvement is associated with aggressive disease and poor prognosis, so early endoscopic evaluation with biopsy can allow for the timely initiation of systemic treatment.
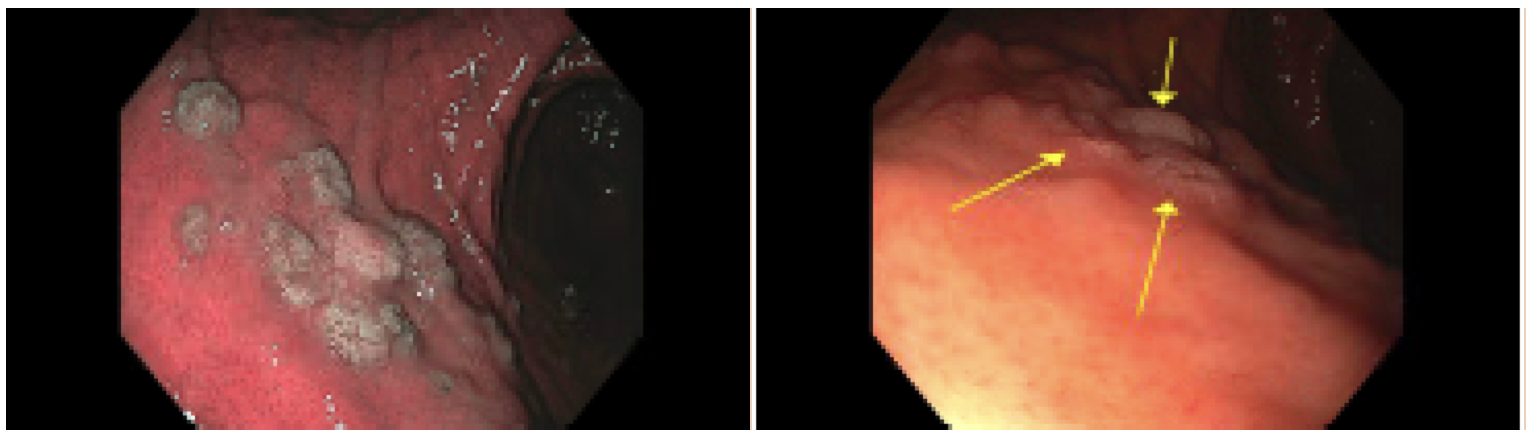
Figure: Figure 1. Multiple small nodules ranging in size from 3-7mm, clustered on the lesser curvature of the stomach. A biopsy was taken with cold forceps for histology.
Disclosures: Isha Bhutada indicated no relevant financial relationships. Samuel Acquah indicated no relevant financial relationships. Serre-Yu Wong: BMS – Advisory Committee/Board Member. Eli Lilly and Company – Grant/Research Support. Takeda/Trinetx – Grant/Research Support.
Isha Bhutada, MD1, Samuel Acquah, MD2, Serre-Yu Wong, MD, PhD1. P5270 - Upper GI Bleed Unveiling Gastric Infiltration by Multiple Myeloma: A Rare Case, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")