University of Texas Health San Antonio San Antonio, TX
Benjamin Heriford, DO, Jason Rocha, MD University of Texas Health San Antonio, San Antonio, TX Introduction: Klippel-Trenaunay syndrome (KTS) is a rare congenital vascular disorder, with prevalence in the United States estimated at 1 in 100,000 people, characterized by capillary malformations, venous malformations, and limb hypertrophy. While typically involving the extremities and cutaneous vasculature, gastrointestinal (GI) manifestations are an underrecognized source of chronic blood loss and iron deficiency anemia. We present a case of a 42-year-old female with KTS who developed significant iron deficiency anemia due to colonic vascular malformations.
Case Description/
Methods: A 42-year-old woman with a known history of KTS and type 2 diabetes mellitus presented for evaluation of iron deficiency anemia. She reported rectal bleeding. Laboratory studies revealed a hemoglobin of 7.4 g/dL and a mean corpuscular volume (MCV) of 76.0 fL. Iron studies were consistent with iron deficiency anemia.
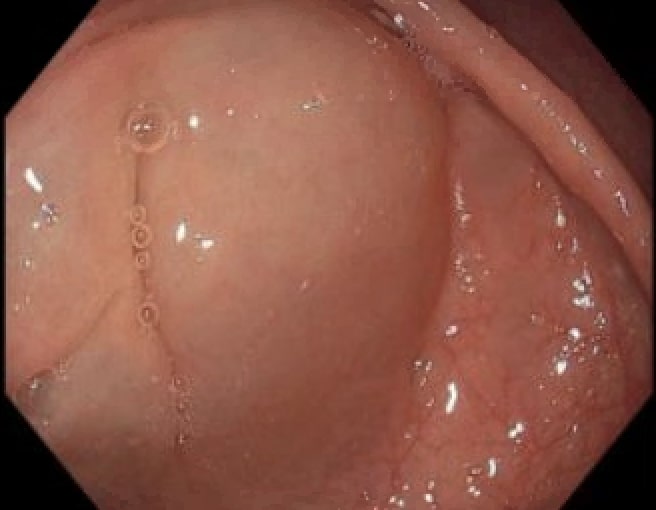
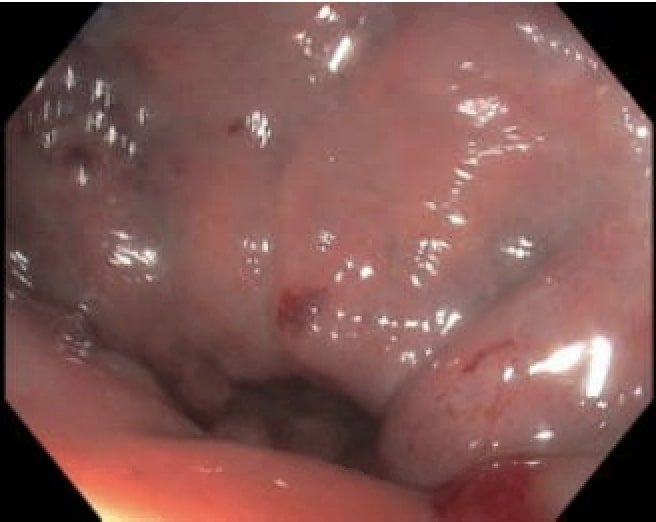
Initial EGD was unremarkable. Colonoscopy revealed numerous subepithelial mucosal blebs, up to 15 mm in size, scattered throughout the colon. Additionally, several patchy rectal angioectasias were identified. Hemostasis was achieved using argon plasma coagulation (APC).
The patient received four doses of intravenous iron with hematology guidance. Her hemoglobin improved to 11.5 g/dL on recheck. Discussion: Literature suggests that risk of developing GI bleeding with KTS ranges from 1-23%. Management of GI bleeding in KTS must be tailored to the extent and severity of vascular malformations. Conservative management includes iron supplementation and transfusions, as appropriate for mild, intermittent bleeding. Endoscopic therapy including argon plasma coagulation, sclerotherapy, and band ligation can be effective for localized lesions and is often considered first-line for bleeding sites amenable to endoscopic intervention. For diffuse or refractory bleeding, interventional radiology techniques such as embolization may be employed.Surgical intervention is reserved for life-threatening or transfusion-dependent bleeding. Options include segmental resection, proctocolectomy, or ultralow anterior resection, with the goal of controlling hemorrhage while preserving function, when possible.
Lessons learned include the importance of early recognition of GI involvement in KTS, the utility of a stepwise, multidisciplinary approach, and the need for long-term follow-up due to the risk of recurrence and complications. Individualized treatment planning is essential to optimize outcomes and minimize morbidity.
Figure: Rectum AVMs and subepitelial blebs.
Figure: Cecal subepitelial bleb.
Disclosures: Benjamin Heriford indicated no relevant financial relationships. Jason Rocha indicated no relevant financial relationships.
Benjamin Heriford, DO, Jason Rocha, MD. P5267 - A Rare Cause of Iron Deficiency Anemia in a Patient With Klippel-Trenaunay Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.