FNU Varsha, MD1, Jahnavi Ethakota, MD1, Bipneet Singh, MD1, Sakshi Bai, MD1, Palak Grover, MD1, Haseeb Khan Tareen, MD1, Fnu Hersha, MD2 1Henry Ford Jackson Hospital, Jackson, MI; 2Jinnah Sindh Medical University, Karachi, Sindh, Pakistan Introduction: Variceal bleeding is a life-threatening complication most commonly associated with cirrhosis-induced portal hypertension. However, non-cirrhotic causes of portal hypertension are increasingly recognized, particularly in younger patients. Among these, splanchnic venous thrombosis (SVT)—which includes thrombosis of the portal, splenic, or mesenteric veins—can lead to the development of ectopic or gastroesophageal varices due to altered venous drainage and increased portal pressure.
We present a case of acute upper gastrointestinal bleeding due to esophageal varices in a patient with non-cirrhotic portal hypertension secondary to splanchnic venous thrombosis, highlighting the diagnostic and therapeutic challenges involved in managing variceal hemorrhage in the absence of liver cirrhosis.
Case Description/
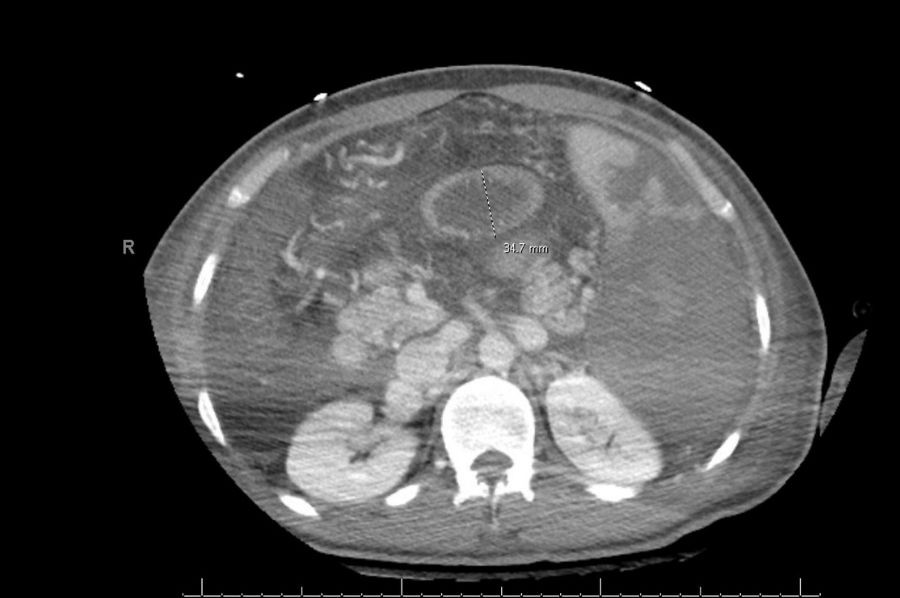
Methods: A 31-year-old male with no past medical history presented with an upper GI bleed and intubated in the ER for airway protection. Initial labs showed leukocytosis WBC 30.85k, anemia Hb 5.7, thrombocytosis 1078K, INR 1.9, fibrinogen 103, and lactate 12. CT abdomen pelvis showed chronic occlusion of the portal and splenic veins with cavernous transformation, and splenomegaly with splenic infarcts is also evident.
He underwent a massive transfusion protocol. He received tranexamic acid, Protonix, octreotide, ceftriaxone, vitamin K. EGD showed gastric varices, underwent gastric and splenic artery embolization and TIPS as well. Hypercoagulable workup positive for JAK2. Autoimmune workup was negative. There is high suspicion of an underlying myeloproliferative disorder given positive JAK-2 mutation and portal vein thrombosis; therefore, an outpatient bone marrow biopsy is recommended by hematology. Discussion: SVT is relatively rare in general population, with an incidence of 0.7 per 100,000 persons per year for portal vein thrombosis. Clinically, portal vein thrombosis may present acutely or chronically. Acute PVT is symptomatic with abdominal pain, fever, or signs of bowel ischemia, and may show a hyperdense thrombus on imaging. In contrast, chronic PVT is often asymptomatic until complications such as portal hypertension or gastrointestinal bleeding occur and usually identified by the presence of cavernous transformation of the portal vein on imaging. Diagnosis begins with Doppler ultrasonography, CT angiography and MRI that assist in identifying thrombus extension, and preferred in cases of suspected chronic PVT. It is important to consider PVT as a potential cause in patients with GI bleed.
Figure: CT abdomen pelvis with IV contrast
Disclosures: FNU Varsha indicated no relevant financial relationships. Jahnavi Ethakota indicated no relevant financial relationships. Bipneet Singh indicated no relevant financial relationships. Sakshi Bai indicated no relevant financial relationships. Palak Grover indicated no relevant financial relationships. Haseeb Khan Tareen indicated no relevant financial relationships. Fnu Hersha indicated no relevant financial relationships.
FNU Varsha, MD1, Jahnavi Ethakota, MD1, Bipneet Singh, MD1, Sakshi Bai, MD1, Palak Grover, MD1, Haseeb Khan Tareen, MD1, Fnu Hersha, MD2. P5263 - The Silent Thrombosis: A Non-Cirrhotic Pathway to Variceal Formation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.