Mercyhealth Gastroenterology Fellowship Rockford, IL
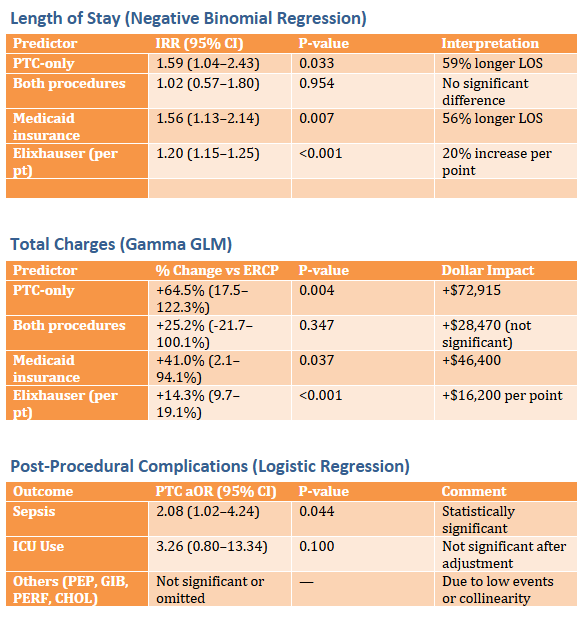
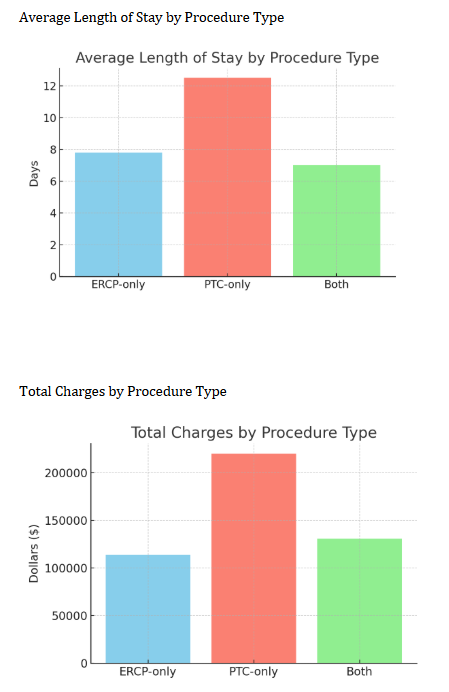
Abu Fahad Abbasi, MD1, Luqman Baloch, MD1, Ahmet Sakiri, MD2, Thayer Hamoudah, MD3, Altaf Dawood, MD3, Naser Khan, MD3, Baseer Qazi, MD3, Jamie Berkes, MD4, Wadih Chacra, MD5, Ashley Vareedayah, MD6 1Mercyhealth Gastroenterology Fellowship, Rockford, IL; 2Mercyhealth Internal Medicine Residency, Rockford, IL; 3Mercyhealth Gastroenterology, Rockford, IL; 4University of Illinois, Chicago, IL; 5University of Illinois College of Medicine, Chicago, IL; 6University of Illinois Hospital, Chicago, IL Introduction: Our study evaluates national in-hospital outcomes in post-liver transplant patients who require ERCP or percutaneous transhepatic cholangiography (PTC) for the treatment of biliary complications, including strictures, leaks, or stones. Methods: National Inpatient Sample data from 2019 to 2021 was utilized to evaluate outcomes for post-liver transplant patients who required ERCP vs. PTC for biliary complications. Liver transplants (both deceased and living donor) & ductal anastomoses of all types were included. Various demographics were assessed including age, biological sex, race, ethnicity, income quartile, & insurance status. Patients were categorized by procedure type utilizing ICD-10 codes. Primary outcomes were hospital length of stay (LOS), total charges, and in-hospital complications (mortality, sepsis, GI bleeding, and ICU use). Multivariate regression models adjusted for demographics and comorbidities helped assess differences in LOS, hospital costs, and in-hospital complications. STATA 19 was used for statistical analysis. P < 0.05 was deemed statistically significant. Results: Of a total of 3,045 weighted hospitalizations, 93.8% underwent an ERCP-only intervention. PTC-only was only 5.8% of patients. Only 0.5% of patients required combined ERCP & PTC. PTC-only had longer LOS (12.5 vs. 7.8 days; P< 0.05) and higher hospital charges ($219,747 vs. $113,832; P=0.004). In-hospital complications such as sepsis were significantly higher in PTC-only (OR 2.08 [1.02–4.24]; P=0.04). Other in-hospital complications such as mortality, ICU use, perforation, & pancreatitis did not differ significantly (P >0.05). When comparing combined ERCP & PTC vs. ERCP-only, there were no statistically significant differences in LOS (P=0.95) or hospital charges (P=0.35). Discussion: ERCP remains the preferred first-line therapy post-liver transplant. PTC use, though infrequent, is linked to 59% longer LOS. PTC use is also noted to have 65% higher costs and an increased risk of sepsis with 2.08 times higher odds of developing sepsis. These disparities may be linked to more anatomically complex biliary complications in post-liver-transplanted patients, necessitating the use of PTC. Limitations of our study include its retrospective design, lack of access to procedural findings, & inability to determine biliary anatomy post-transplant (duct-to-duct anastomosis vs. Roux-en-Y choledochojejunostomy). Despite these limitations, the large sample size & multivariate analysis strengthen our findings.
Figure: Tables of Outcomes for Length of Stay, Total Charges, & Post-Procedural Complications.
Figure: Bar Graphs Depicting Average Length of Stay & Total Charges by Procedure Type.
Disclosures: Abu Fahad Abbasi indicated no relevant financial relationships. Luqman Baloch indicated no relevant financial relationships. Ahmet Sakiri indicated no relevant financial relationships. Thayer Hamoudah indicated no relevant financial relationships. Altaf Dawood indicated no relevant financial relationships. Naser Khan indicated no relevant financial relationships. Baseer Qazi indicated no relevant financial relationships. Jamie Berkes indicated no relevant financial relationships. Wadih Chacra indicated no relevant financial relationships. Ashley Vareedayah indicated no relevant financial relationships.
Abu Fahad Abbasi, MD1, Luqman Baloch, MD1, Ahmet Sakiri, MD2, Thayer Hamoudah, MD3, Altaf Dawood, MD3, Naser Khan, MD3, Baseer Qazi, MD3, Jamie Berkes, MD4, Wadih Chacra, MD5, Ashley Vareedayah, MD6. P5677 - National In-Hospital Outcomes in Biliary Complications Post-Liver Transplant: ERCP vs. PTC, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.