P5753 - Combined Antegrade and Retrograde Endoscopic Dilation Technique with Controlled Recanalization of Complete Esophageal Obstruction from Upper Esophageal Stricture
Carlos Vega-Mena, MD1, Rene Gomez-Esquivel, MD2, Pratik Patel, MD1, Rishi Bolla, MD1 1USF Health, Tampa, FL; 2University of South Florida Morsani College of Medicine, Tampa, FL Introduction: Complete esophageal obstruction (CEO) is a rare cause of esophageal strictures. Standard dilation techniques are not usually feasible due to altered esophageal anatomy and higher complication rates (1). The most common cause of CEO is radiation therapy for cancer. Combined antegrade and retrograde endoscopic dilation (CARD) has a technical success rate of 89% and dysphagia improvement rate of 58.4% (2). We present a case of luminal restoration of CEO with CARD.
Case Description/
Methods: A 68-year-old-male with a history of radiation treatment for laryngeal cancer presented for esophagogastroduodenoscopy (EGD) with CARD for luminal restoration. He reported severe dysphagia and odynophagia for the past 2 years and relied on a percutaneous gastrostomy (PEG) tube for feeds. Modified barium swallow showed a complete luminal obstruction at the upper esophagus. Given inability to traverse the upper esophageal stenosis with a pediatric antegrade endoscope, we proceeded to remove the existing 20 Fr PEG tube and pass a pediatric endoscope in retrograde fashion into the esophagus. A dilator wire was unable to pass through a complete obstruction at the proximal esophagus. Using the pediatric upper endoscope advanced in an antegrade fashion, a Savary guide wire was advanced, unable to pass through the stricture. Using the pediatric forceps, the thin mucosa was sheared retrograde and the Savary wire was grasped and left in the stomach. The patient then underwent anterograde bougie cap dilation of 7-8 mm followed by 9-10 mm using the upper endoscope. The stenosis was able to be traversed, followed by serial dilations with luminal restoration. Discussion: Several endoscopic procedures have been documented for recanalization of CEO. Including antegrade approach with traumatic forward probing and luminal dilation with fluoroscopy (3). CARD is preferred due to success rates and favorable safety profile over sole antegrade approach (3). This case shows the effectiveness of CARD in cases of CEO failing standard dilation techniques.
References 1.Hayat, et al. Combined antegrade and retrograde dilation (CARD) for management of complete esophageal obstruction: Multicenter case series. 2024 Oct 15;12(10):E1199–E1205.
2. Jayaraj, et al. Safety and efficacy of combined antegrade and retrograde endoscopic dilation for complete esophageal obstruction: a systematic review and meta-analysis. 2019 Jul-Aug;32(4):361-369.
3. Vitali, et al. Endoscopic recanalization of complete esophageal obstruction. 2021 Jun;35(6):3184-3188.
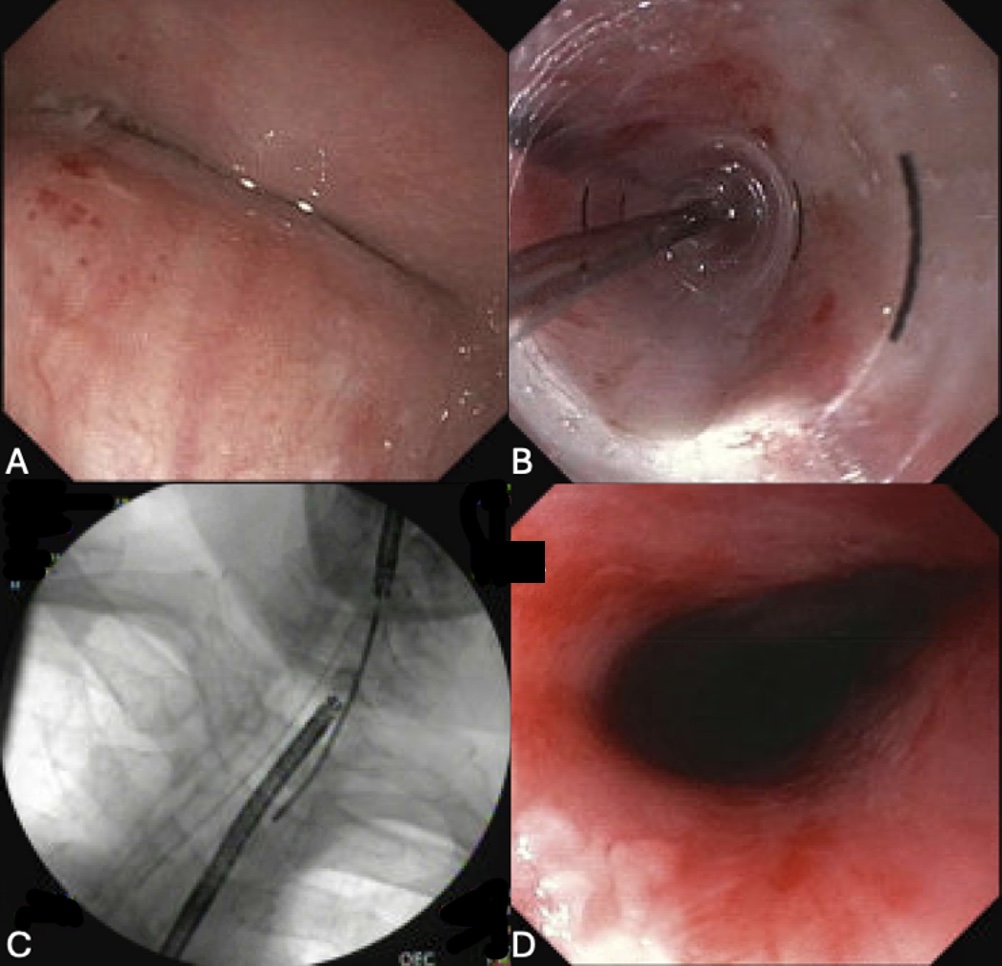
Figure: Figure 1: A) EGD view of stricture at upper third of the esophagus. B) EGD with wire dilation through stricture. C) Fluoroscopy view of upper and lower endoscopes. D) Upper third of the esophagus, post dilation.
Disclosures: Carlos Vega-Mena indicated no relevant financial relationships. Rene Gomez-Esquivel indicated no relevant financial relationships. Pratik Patel indicated no relevant financial relationships. Rishi Bolla indicated no relevant financial relationships.
Carlos Vega-Mena, MD1, Rene Gomez-Esquivel, MD2, Pratik Patel, MD1, Rishi Bolla, MD1. P5753 - Combined Antegrade and Retrograde Endoscopic Dilation Technique with Controlled Recanalization of Complete Esophageal Obstruction from Upper Esophageal Stricture, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.