University of Virginia Medical Center Charlottesville, VA
Manavi Bhagwat, MD1, Nicholas Koutlas, MD1, Neha Rajpal, MD1, Alexander Podboy, MD2 1University of Virginia Medical Center, Charlottesville, VA; 2University of Virginia Health, Charlottesville, VA Introduction: Gallstone ileus is an uncommon cause of bowel obstruction and can occur in patients that develop cholecystoenteric fistulas. Colonic obstruction from gallstones accounts for approximately 4% of all cases of gallstone ileus. Predisposing factors include female sex, older age, and diverticular disease. Typically, it is managed surgically with enterolithotomy, fistula resection, and cholecystectomy. In poor surgical candidates, endoscopic modalities, including mechanical and electrohydraulic lithotripsy (EHL), have been described as primary therapy. We present a case of gallstone mediated obstruction in the sigmoid colon managed endoscopically with electrohydraulic lithotripsy (EHL) prior to surgery.
Case Description/
Methods: An 80-year-old woman with known sigmoid diverticulosis presented with severe abdominal pain, distention, and inability to pass flatus. Computerized tomography (CT) revealed chronic cholecystocolonic fistula at the hepatic flexure with an impacted 4.2 cm gallstone in the sigmoid colon. Colorectal surgery was consulted and they requested endoscopic management to optimize the patient prior to surgery. Flexible sigmoidoscopy revealed extensive sigmoid diverticulosis and a large gallstone impacted into the wall of the sigmoid colon with surrounding shallow mucosal ulceration and hyperemia. EHL was conducted using three probes and 2190 pulses, resulting in successful fragmentation of the stone. Saline irrigation was then utilized to flush stone debris distally. Due to severe diverticular disease and fecal material, the cholecystocolonic fistula was not reachable endoscopically. Following the procedure, the patient reported improvement in pain with passage of flatulence and bowel movements. Four days post-procedure, she underwent elective right hemicolectomy with fistula takedown, sigmoid colectomy, diverting loop ileostomy creation, and subtotal cholecystectomy. She has recovered well and reported no symptoms at her postoperative visit. She has a follow up visit with colorectal surgery to discuss ileostomy takedown. Discussion: In this case, endoscopic therapy with EHL allowed for a more optimized surgical intervention and avoided urgent surgery, which carries increased risk in elderly patients. This case adds to literature that suggests EHL of gallstone colonic obstruction is safe and can be a valuable adjunct to surgery.
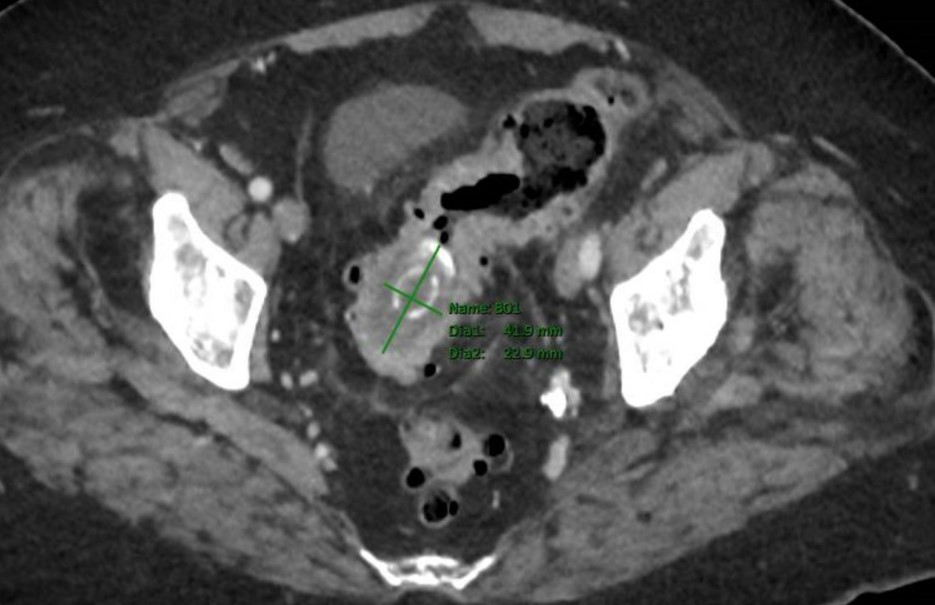
Figure: Figure 1. A 4.2 cm gallsone in sigmoid colon at the level of chronic wall thickening from chronic diverticulitis.
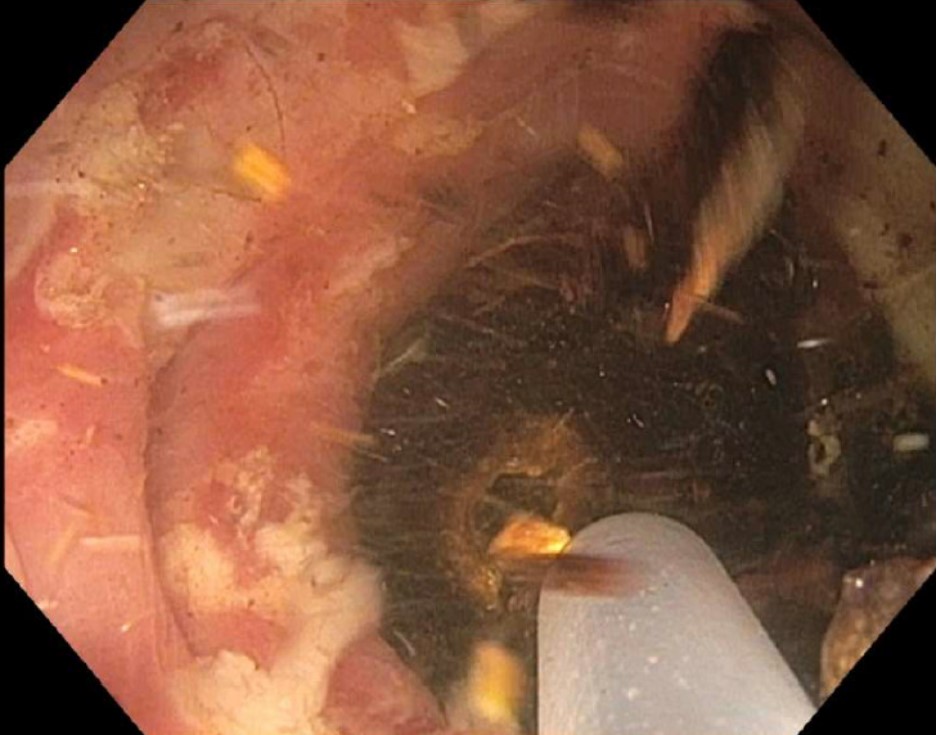
Figure: Figure 2. EHL of gallstone in sigmoid colon.
Disclosures: Manavi Bhagwat indicated no relevant financial relationships. Nicholas Koutlas indicated no relevant financial relationships. Neha Rajpal indicated no relevant financial relationships. Alexander Podboy indicated no relevant financial relationships.
Manavi Bhagwat, MD1, Nicholas Koutlas, MD1, Neha Rajpal, MD1, Alexander Podboy, MD2. P5752 - Sending Shockwaves Through the Colon: Electrohydraulic Lithotripsy of Obstructing Colonic Gallstone Prior to Surgery, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.