Lindsey A. Creech, DO, MBA, MPH, Abdillahi Ahmed, MD, Tiffany Chua, MD University of Florida, Gainesville, FL Introduction: Formal guidelines on the management of intradiverticular polyps have yet to be established. Endoscopic removal of these polyps poses an increased risk of perforation and incomplete resection. This case series describes two patients with intradiverticular polyps successfully removed without complication via combined endoscopic mucosal resection (EMR) and endoscopic full-thickness resection (EFTR).
Case Description/
Methods: Case One: A 79-year-old male was evaluated for a recurrent villous adenoma with high grade dysplasia in the descending colon despite three piecemeal polypectomies in the preceding year. Colonoscopy revealed a 25 mm sessile polyp emerging from a diverticulum in the descending colon. Cold endoscopic mucosal resection was performed to debulk the extra-diverticular portion of the polyp in piecemeal fashion. Pathology was consistent with TVA. The patient was referred for EFTR with full-thickness resection device (FTRD) to complete the resection one month later. Final pathology was negative for dysplasia. Due to his age, the patient declined further surveillance.
Case Two: A 72-year-old male with prostate cancer underwent colonoscopy to investigate radiotracer uptake within the colon on positron emission tomography scan. Multiple polyps, including one 35 mm tubulovillous adenomas (TVA) and one 15 mm tubular adenoma (TA) with high grade dysplasia, were found throughout the colon. Poor bowel prep secondary to pandiverticulosis halted initial removal. Repeat sigmoidoscopy revealed a 35 mm and 15 mm polyp in the sigmoid colon involving diverticula. Underwater EMR via hot snare was used to debulk the extra-diverticular portion of the 35 mm polyp in piecemeal fashion. EFTR with FTRD was then used to remove the central, intradiverticular portion of the polyp. The 15 mm polyp was removed similarly during flexible sigmoidoscopy three months later. Follow-up endoscopies showed post-EMR scars negative for recurrent disease. Discussion: As the prevalence of diverticulosis and polyps increase with age and the western diet, we may encounter more patients with intradiverticular polyps. Our experience suggests a hybrid approach of debulking EMR followed by EFTR with FTRD to removal residual polyp within a diverticulum is feasible and has an acceptable safety profile for both rescue and primary therapy of colonic lesion involving diverticula.
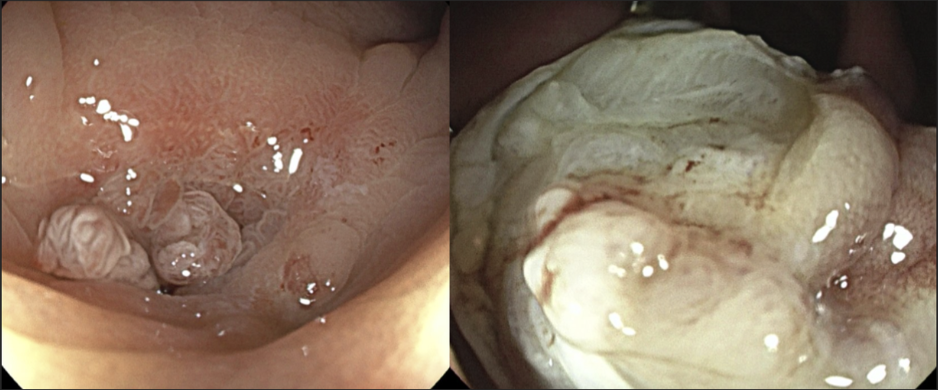
Figure: Figure 1. Case 1. A 25 mm sessile polyp emerging from a diverticulum in the descending colon (left), and the resection site after EMR followed by EFTR with FTRD (right).
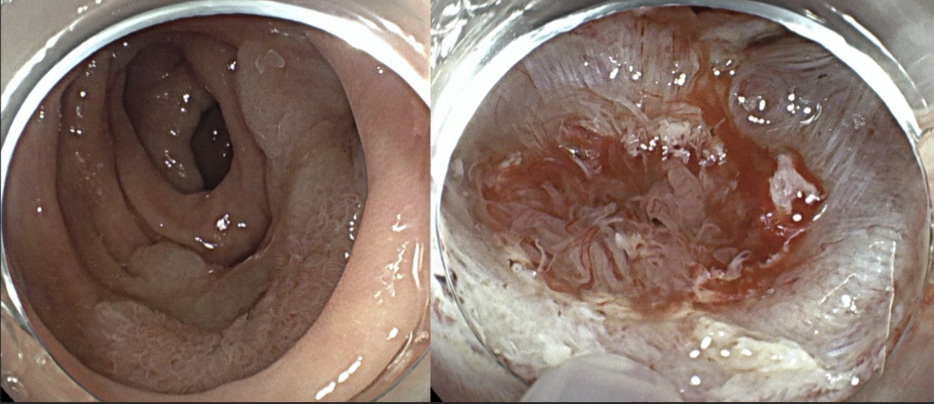
Figure: Figure 2. Case 2. A 35 mm polyp within a diverticulum in the sigmoid colon (left), and the resection site after debulking EMR immediately before FTRD (right).
Disclosures: Lindsey Creech indicated no relevant financial relationships. Abdillahi Ahmed indicated no relevant financial relationships. Tiffany Chua indicated no relevant financial relationships.
Lindsey A. Creech, DO, MBA, MPH, Abdillahi Ahmed, MD, Tiffany Chua, MD. P5738 - Navigating Challenges in Colonic Diverticular Polypectomy: EMR and EFTR With FTRD for an Interdiverticular Adenoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.