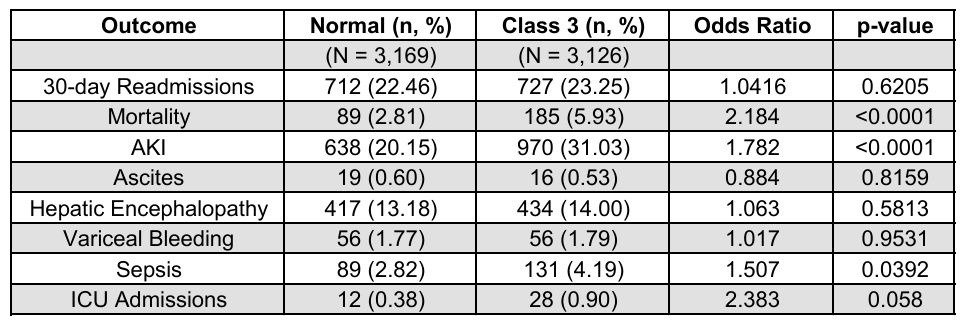
Muaataz Azzawi, MD1, Medha Rajamanuri, MD2, Muhammed Yaman Swied, MBBS1, Steven Scaife, MS1, Ahmed Al-Khazraji, MD3, Abdul Swied, MD1 1Southern Illinois University, Springfield, IL; 2Medha Rajamanuri, Springfield, IL; 3Rutgers New Jersey Medical School, Newark, NJ Introduction: Obesity is increasingly recognized as an important modifier of disease severity and prognosis in alcohol-associated hepatitis (AH). The recently defined entity of metabolic dysfunction–associated alcohol-related liver disease (MetALD) highlights patients with overlapping metabolic and alcohol-related risk factors who may be at particularly high risk for adverse outcomes. This retrospective study aims to investigate the association between obesity and various clinical outcomes in hospitalized patients with alcohol-associated hepatitis. Methods: We utilized the Nationwide Readmission Database (NRD), Healthcare Cost and Utilization Project (HCUP), and Agency for Healthcare Research and Quality (AHRQ) to identify patients diagnosed with alcohol-associated hepatitis between 2016 and 2021 using ICD-10 codes. Patients were categorized into normal weight, class I, class II, and class III obesity groups based on BMI recorded closest to the time of diagnosis. We assessed outcomes for each obesity category versus normal-weight patients, including 30-day readmission, mortality, acute kidney injury (AKI), decompensation events (ascites, esophageal bleeding, or hepatic encephalopathy), sepsis, ICU admissions, and need for mechanical ventilation. A total of 8,739 obese patients were analyzed and matched with 8,981 normal-weight patients based on gender, age, ethnicity, and comorbidities to reduce confounders. Results: Our study demonstrated a higher likelihood of acute kidney injury (AKI) in patients with class 3 obesity compared to those with normal weight, with rates of 31.03% vs. 20.15% (OR 1.70, P < 0.001). Additionally, there was a significant increase in mortality among patients with class 3 obesity (5.93% vs. 2.81%, OR 2.81, P < 0.001). The likelihood of sepsis was also higher in the class 3 obesity group compared to normal-weight individuals (4.19% vs. 2.82%, OR 1.51, P < 0.039). ICU admissions were noticeably higher in the class 3 obesity group, but it was not clinically significant (0.9% vs. 0.39%, OR 2.38, P < 0.058).
Discussion: Class 3 obesity is associated with increased rates of acute kidney injury, mortality, and sepsis in patients hospitalized with alcohol-associated hepatitis. These findings underscore the role of class 3 obesity as an important modifier in the clinical course of alcohol-associated liver disease and highlight the need for targeted interventions and risk stratification strategies in this high-risk population.
Figure: Table: Inpatient Outcomes – Normal vs Class 3
Disclosures: Muaataz Azzawi indicated no relevant financial relationships. Medha Rajamanuri indicated no relevant financial relationships. Muhammed Yaman Swied indicated no relevant financial relationships. Steven Scaife indicated no relevant financial relationships. Ahmed Al-Khazraji indicated no relevant financial relationships. Abdul Swied indicated no relevant financial relationships.
Muaataz Azzawi, MD1, Medha Rajamanuri, MD2, Muhammed Yaman Swied, MBBS1, Steven Scaife, MS1, Ahmed Al-Khazraji, MD3, Abdul Swied, MD1. P5921 - Impact of Obesity on Outcomes in Patients Presenting With Alcohol-Associated Hepatitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.