Université Paris Cité, UMR1149 (CRI), INSERM Paris, Ile-de-France, France
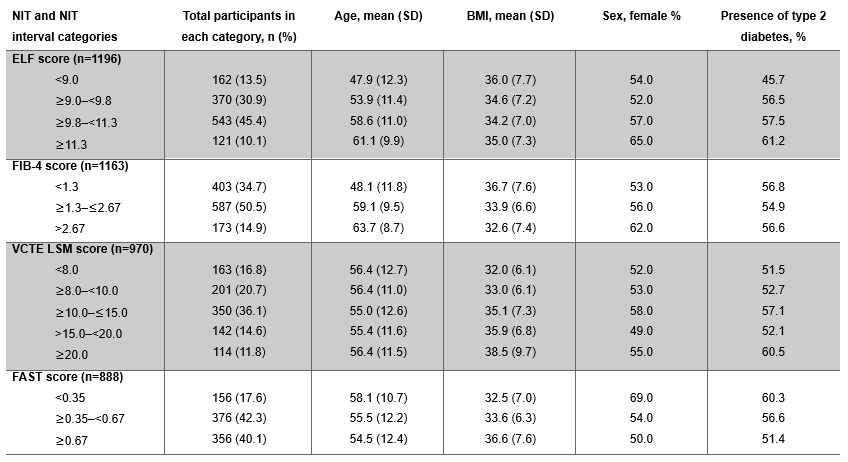
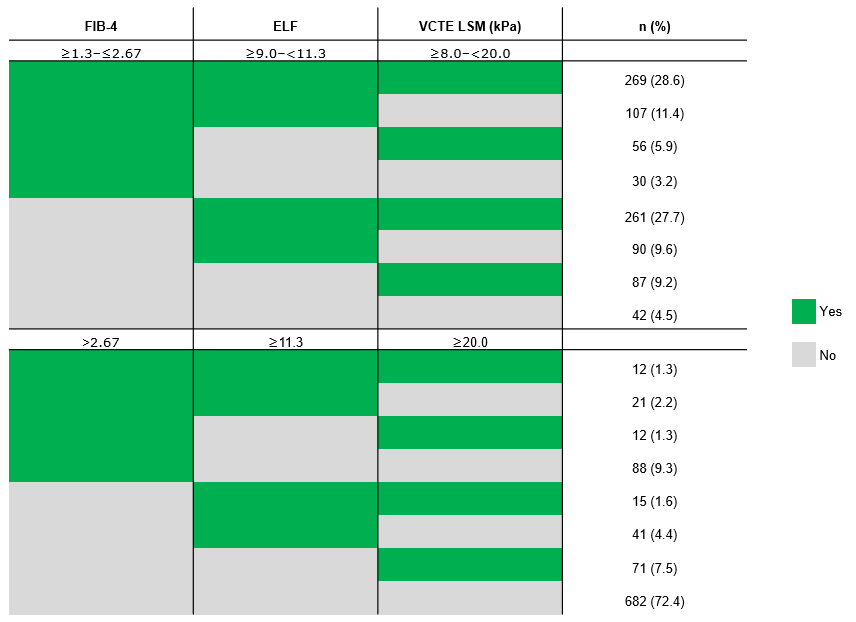
Laurent Castera, MD, PhD1, Kristiane Engebretsen, MD, PhD2, George B.. Goh, MBBS, MRCP (UK), M Med (Int Med), FAMS (Singapore)3, Elisabetta Bugianesi, MD, PhD4, Anna M.G.. Calí, MD, MSc2, Burak Demirel, MD2, Tomáš Koller, MD, PhD5, Niels Krarup, MSc2, Michelle T.. Long, MD, MSc2, Philip Newsome, MD, PhD6, Cláudia Oliveira, MD, PhD7, Vlad Ratziu, MD, PhD8, Mary E.. Rinella, MD9, Michael Roden, MD, PhD10, Giada Sebastiani, MD11, Arun J.. Sanyal, MD12 1Université Paris Cité, UMR1149 (CRI), INSERM, Paris, Ile-de-France, France; 2Novo Nordisk A/S, Copenhagen, Hovedstaden, Denmark; 3Department of Gastroenterology and Hepatology, Singapore General Hospital, Singapore, Singapore; 4Department of Medical Sciences, University of Turin, Turin, Piemonte, Italy; 5Subdivision of Gastroenterology and Hepatology, 5th Department of Internal Medicine, Comenius University Faculty of Medicine, University Hospital Bratislava, Bratislava, Bratislava, Slovakia; 6Roger Williams Institute of Liver Studies, Faculty of Life Sciences and Medicine, King’s College London and King’s College Hospital, London, England, United Kingdom; 7Departamento de Gastroenterologia, Hospital das Clínicas (LIM07) da Faculdade de Medicina da Universidade de São Paulo, Sao Paulo, Sao Paulo, Brazil; 8Sorbonne Université, Institute for Cardiometabolism and Nutrition, Hospital Pitié Salpêtrière, INSERM UMRS 1138 CRC, Paris, Ile-de-France, France; 9Division of Gastroenterology, Hepatology and Nutrition, University of Chicago, Chicago, IL; 10Department of Endocrinology and Diabetology, Medical Faculty and University Hospital Düsseldorf, Heinrich Heine University Düsseldorf, Dusseldorf, Nordrhein-Westfalen, Germany; 11Division of Gastroenterology and Hepatology, McGill University Health Centre, Montreal, PQ, Canada; 12Virginia Commonwealth University; Central Virginia Veterans Healthcare System, Richmond, VA Introduction: ESSENCE is an ongoing phase 3 trial (NCT04822181) in participants with biopsy-defined, non-cirrhotic metabolic dysfunction-associated steatohepatitis (MASH).In part 1, the primary histological endpoints were met in the first 800 randomised participants after 72 weeks’ treatment with semaglutide 2.4 mg. The aim of this post hoc analysis was to characterise the total randomised, baseline population using selected non-invasive tests (NITs). Methods: Randomised participants (N=1197) were characterised by NITs at baseline: vibration-controlled transient elastography liver stiffness measurement (VCTE LSM; FibroScan), enhanced liver fibrosis (ELF) score, FibroScan-aspartate aminotransferase (FAST) score and Fibrosis-4 index (FIB-4) score. Eligible participants had histologically defined MASH and liver fibrosis stage 2 or 3. Clinical NIT categories for moderate-to-advanced fibrosis were used to group participants, and descriptive statistics determined numbers of participants in each NIT category and demographics. Results: Distribution of results is shown in Table 1. At baseline, 95.5% fulfilled NIT scores in ≥1 of the guideline-recommended ranges for FIB-4 (≥1.3–≤2.67), ELF (≥9.0–< 11.3) or VCTE LSM (≥8.0–< 20.0 kPa) (Table 2). Most had a FAST score ≥0.35 (82.4%) and 34.7% had a FIB-4 score < 1.3 (Table 1). As expected, participants with FIB-4 score < 1.3 were younger (mean age: 48.1 years) than those with FIB-4 score ≥1.3–≤2.67 (59.1 years) and >2.67 (63.7 years). They also had a higher mean BMI (36.7 kg/m2) and were more likely to be men than those with FIB-4 score ≥1.3. Of those with a baseline FIB-4 measurement outside the guideline-recommended category for moderate-to-advanced fibrosis (n=480), 91.3% had other NITs within the guideline-recommended category (ELF score ≥9.0–< 11.3 or VCTE LSM ≥8.0–< 20.0 kPa) (Table 2). Of note, 27.6% of participants had ≥1 NIT score that was above the guideline-recommended limit, however, only 1.3% had values above the upper limits of all NITs (Table 2). Additionally, those with VCTE LSM scores ≥20.0 kPa had a higher mean BMI (38.5 kg/m2) and were more likely to have type 2 diabetes (61.0%) than those with VCTE LSM < 20.0 kPa (Table 1). Discussion: While participants in ESSENCE had biopsy-defined stage 2 or 3 fibrosis, the population had a broad range of NIT values. If there is a clinical suspicion for MASH with moderate fibrosis, use of multiple NITs may support a clinical diagnosis of MASH.
Figure: Table 1. Baseline NIT score groupings in those with a recorded measurement in the ESSENCE randomized population (N=1197). BMI, body mass index; ELF, enhanced liver fibrosis; FAST, FibroScan-AST; FIB-4; Fibrosis-4; NIT, non-invasive test; SD, standard deviation; VCTE LSM, vibration-controlled transient elastography liver stiffness measurement.
Figure: Table 2. NIT cutoff cross table in those with histologically confirmed fibrosis stage 2 or 3 and with a baseline measurement in reported NITs (N=942). ELF, enhanced liver fibrosis; FIB-4, Fibrosis-4; NIT, non-invasive test; VCTE LSM, vibration-controlled transient elastography liver stiffness measurement.
Laurent Castera, MD, PhD1, Kristiane Engebretsen, MD, PhD2, George B.. Goh, MBBS, MRCP (UK), M Med (Int Med), FAMS (Singapore)3, Elisabetta Bugianesi, MD, PhD4, Anna M.G.. Calí, MD, MSc2, Burak Demirel, MD2, Tomáš Koller, MD, PhD5, Niels Krarup, MSc2, Michelle T.. Long, MD, MSc2, Philip Newsome, MD, PhD6, Cláudia Oliveira, MD, PhD7, Vlad Ratziu, MD, PhD8, Mary E.. Rinella, MD9, Michael Roden, MD, PhD10, Giada Sebastiani, MD11, Arun J.. Sanyal, MD12. P5830 - The Use of Non-Invasive Tests to Characterise the Total Baseline Population in the Phase 3 Essence Trial, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.