University of Arkansas for Medical Sciences Little Rock, AR
Suria Devarapalli, DO1, Srikanth Vallurupalli, MD2, Ragesh Thandassery, MD3 1University of Arkansas for Medical Sciences, Little Rock, AR; 2Central Arkansas Veterans Healthcare System, Little Rock, AR; 3Central Arkansas Veterans Healthcare System, University of Arkansas for Medical Sciences, Little Rock, AR Introduction: Baveno VII criteria recommend vibration-controlled transient elastography (FibroScan) to diagnose compensated advanced chronic liver disease (cACLD) and clinically significant portal hypertension (CSPH). However, FibroScan is not widely available in primary care and resource limited settings. We aimed to compare the accuracy of easily available blood-based noninvasive tests (NITs) to predict cACLD, CSPH and hepatic steatosis (HS). Methods: In a US veteran cohort (n=1298, referred from primary care to liver clinic between 2017 and 2024), we compared the NITs- APRI, FIB-4 score, NAFLD fibrosis score (NFS) with cACLD and CSPH (FibroScan-liver stiffness measurement and platelet count). We also compared another NIT, hepatic steatotic index (HSI) with FibroScan-continued attenuation parameter (CAP). HS was defined as CAP ≥288dB/m. Results: Mean age was 61.2 (+11.4) years (91% males; 68.4% Caucasians, 44.1% MASLD, 31.1% chronic hepatitis C). Median BMI was 30.3 (25.9-35). cACLD was present in 14.3%, CSPH in 5.5%, and HS in 52.7%.
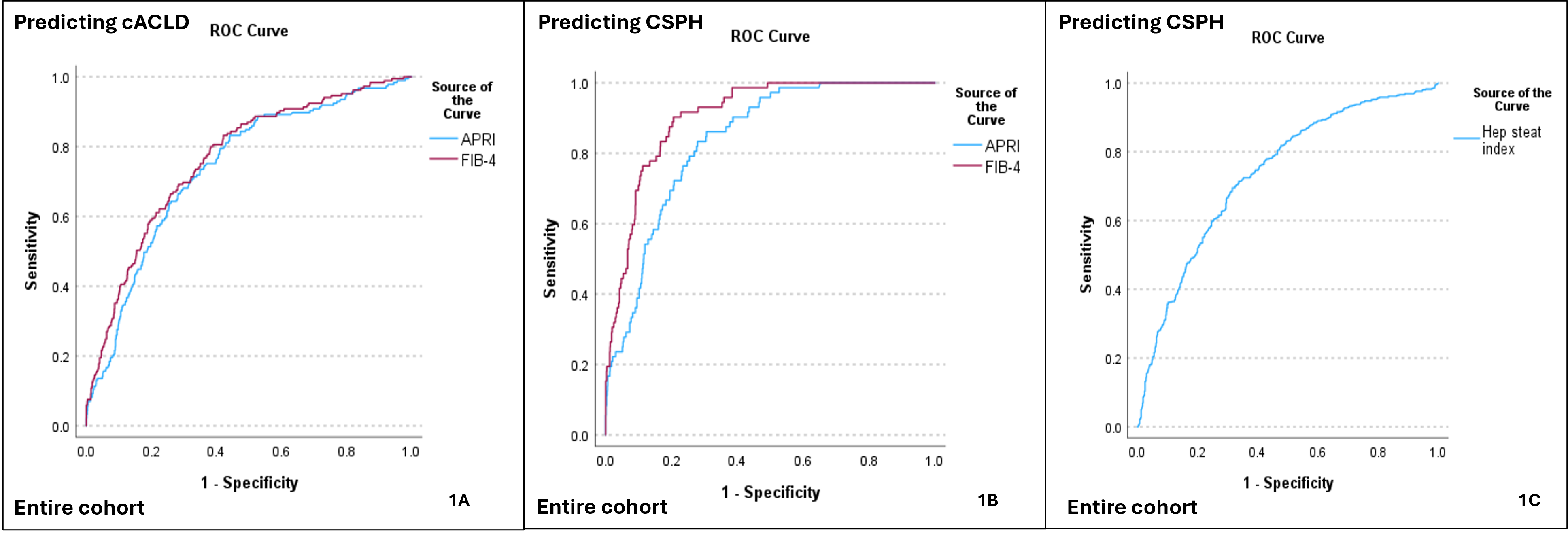
The predictive accuracy (AUROCs [±SE]) of FIB-4 and APRI for cACLD were 0.788 (0.029) and 0.738 (0.019) and for CSPH were 0.907 (0.013) and 0.839 (0.019) respectively (Figure-1). At a cut-off of 3.25, FIB-4 had 77.1% sensitivity and 85.2% specificity for predicting cACLD (p=0.001), and 76.4% sensitivity and 88.2 % specificity for predicting CSPH (p=0.001).
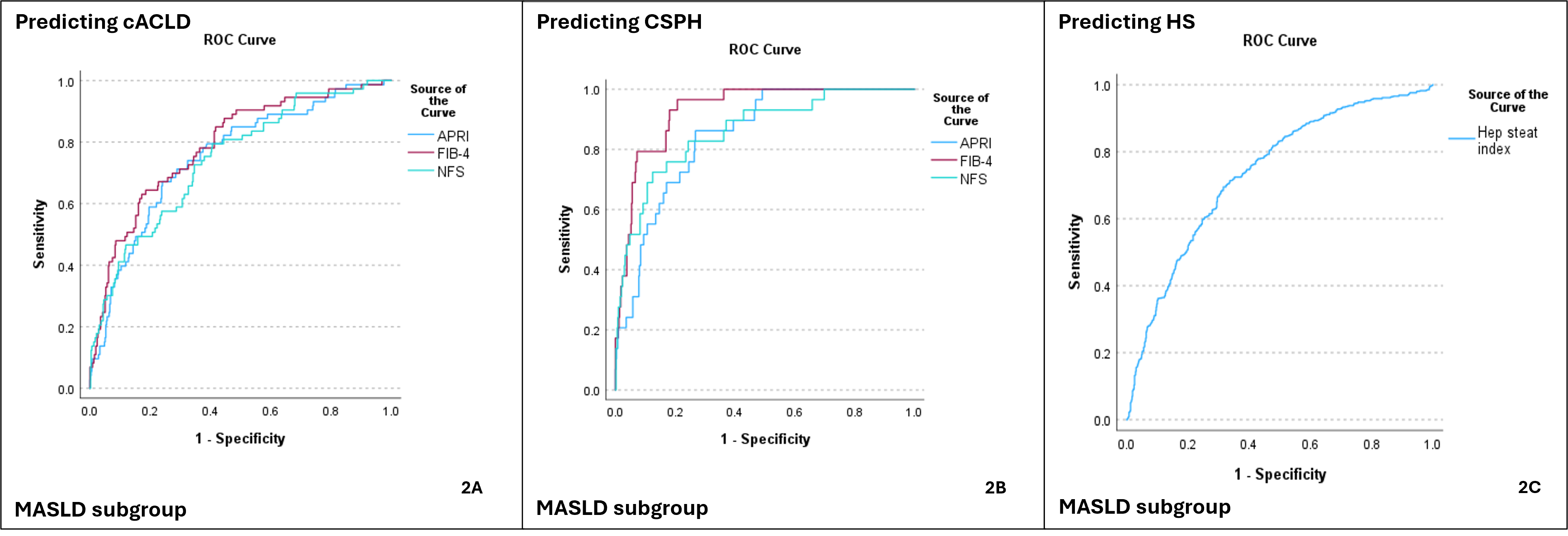
In subgroup analysis of patients with MASLD, the AUROC (SE) for FIB-4, APRI and NFS for predicting cACLD were 0.788 (0.029), 0.753 (0.031) and 0.743 (0.031) and for predicting CSPH were 0.931 (0.017), 0.846 (0.029) and 0.862 (0.036) respectively. At a cut-off of 2.67, FIB-4 had 79.2% sensitivity and 85.2% specificity for predicting cACLD (p=0.001) and 79.3% sensitivity and 84.0 % specificity for predicting CSPH (p=0.001).
For predicting HS, the HSI at cut-off 36 had 81% sensitivity and 53% specificity, p=0.001 (AUROC 0.677 [0.027]). In MASLD subgroup, HSI had 91.8 % sensitivity and 64.1% specificity, p=0.001 (AUROC of 0.763 [0.019]) with the same cut-off. Discussion: NITs identified patients with cACLD and CSPH with acceptable and good predictive accuracy respectively. Among the NITs, FIB-4 had the highest accuracy for predicting cACLD and CSPH, irrespective of etiology of liver disease. Similarly, HSI had acceptable accuracy for identifying hepatic steatosis in MASLD. NITs can help identify and expedite referral of high-risk patients (with cACLD and CSPH) to specialized liver clinics.
Figure: Title Accuracy of NITs for Predicting cACLD, CSPH and hepatic steatosis (for entire cohort) Legend NITs- noninvasive tests, ROC= Receiver Operating Characteristic, Hepatic steatotic index (HSI) = 8 x (ALT/AST) + BMI + (2 if female) + (2 if diabetes)
Figure: Accuracy of NITs for Predicting cACLD, CSPH and hepatic steatosis (for MASLD subgroup)
Disclosures: Suria Devarapalli indicated no relevant financial relationships. Srikanth Vallurupalli indicated no relevant financial relationships. Ragesh Thandassery indicated no relevant financial relationships.
Suria Devarapalli, DO1, Srikanth Vallurupalli, MD2, Ragesh Thandassery, MD3. P5779 - Performance of Blood-Based Noninvasive Tests (NITs) in Predicting cACLD and CSPH to Facilitate Referral to Liver Clinics, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.