Rukmoni Balasubramanian, MBBS1, Anjali Rajagopal, MBBS2, Vaibhav Mehendiratta, MD3 1University of Connecticut, Farmington, CT; 2University of Connecticut Health Center, Farmington, CT; 3Hartford Hospital, Hartford, CT Introduction: Bouveret syndrome predominantly occurs in elderly women with a long-standing history of gallstones. It is characterized by gallstone impaction in the pylorus or duodenum secondary to a cholecystoduodenal or cholecystogastric fistula. CT imaging is highly sensitive, and evidence of pneumobilia, small bowel obstruction and an ectopic gallstone (Rigler’s triad) should prompt consideration of this condition.
Case Description/
Methods: An 89-year-old female with a medical history of hypertension and prior small bowel obstruction managed conservatively presented with abdominal pain and decreased oral intake. Prior imaging had incidentally revealed a large gallstone within a moderately distended gallbladder. Non-contrast CT of abdomen and pelvis demonstrated a cholecystoduodenal fistula with the gallstone now located within the duodenum, along with evidence of periduodenal fluid stranding and air in gallbladder.
An esophagogastroduodenoscopy (EGD) was performed for stone removal. Endoscopic evaluation revealed a large cholecystoduodenal fistula in the duodenal bulb. A large gallstone impacted in the duodenum, consistent with Bouveret Syndrome, was identified. The stone was slowly fragmented and removed using a combination of mechanical and electrohydraulic lithotripsy (EHL). The patient was transitioned to a clear liquid diet post-procedure and monitored for clinical improvement. Discussion: Bouveret syndrome is a rare form of gallstone ileus, accounting for only 1–3% of cases. This syndrome involves gastric outlet obstruction due to an impacted gallstone, making it uncommon and challenging to manage. Endoscopic therapy is the preferred approach in high-risk surgical candidates, while operative management remains an option when endoscopic attempts fail.
We present a complex case requiring multiple advanced endoscopic techniques. Initial efforts using a snare, rescue net, and lithotripsy basket were unsuccessful. EHL was subsequently employed and required three probes over two hours to achieve adequate stone fragmentation. The procedure was further complicated by distal stone migration and impaction at the ligament of Treitz. Mechanical lithotripsy was ultimately successful in achieving complete stone removal.
While endoscopic success rates for Bouveret syndrome are variable (range from 10% to 40%), this case highlights the feasibility and effectiveness of combining multiple minimally strategies from biliary toolbox to achieve desired outcome in elderly patients with multiple comorbidities.
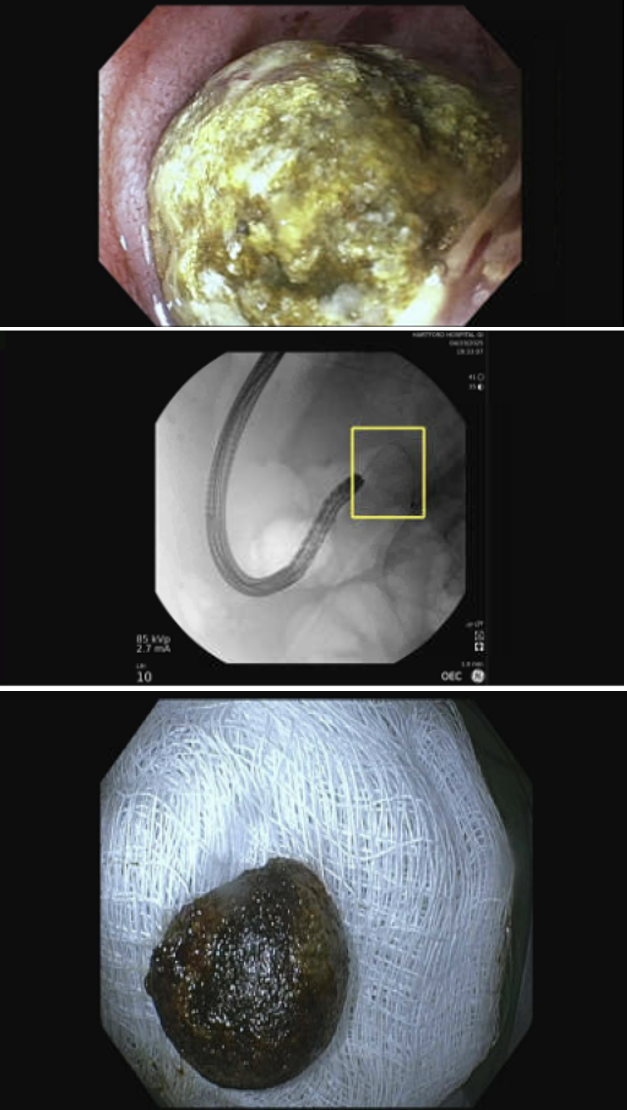
Figure: Figure 1: Fistula noted in duodenal bulb
Figure: Figure 2.1, 2.2 and 2.3: Impacted Stone
Disclosures: Rukmoni Balasubramanian indicated no relevant financial relationships. Anjali Rajagopal indicated no relevant financial relationships. Vaibhav Mehendiratta indicated no relevant financial relationships.
Rukmoni Balasubramanian, MBBS1, Anjali Rajagopal, MBBS2, Vaibhav Mehendiratta, MD3. P5721 - Bouveret Syndrome Managed Endoscopically via Electrohydraulic and Mechanical Lithotripsy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")