Usman Rahim, MD1, Bukhtawar Munir, MD2, Dragos Pausescu, MD2, Johnson Yeboah, MD3 1Adventist Health System, Hanford, CA; 2Adventist Health, Hanford, CA; 3Adventist Health, Tulare, CA Introduction: Gastric perforation involves full thickness injury to the wall. It carries a very high-risk mortality in patients with decompensated liver disease and acute liver failure. Patients have been historically managed with surgical intervention to prevent further leakage of gastrointestinal contents, risk of peritonitis and abscess formation. Alternative approach includes endoscopic repair.
Case Description/
Methods: 66-year-old male patient with past medical history of morbid obesity who presented with worsening abdominal pain of three days duration. Abdominal imaging was significant for cirrhotic liver and gastric perforation. The patient underwent emergent laparotomy and gastric perforation was managed with Graham patch repair. The patient was started on a clear liquid diet. However, on postoperative day nine, his pain reoccurred, and he developed purulent output from Jackson-Pratt drain. Upper gastrointestinal (GI) series was performed which confirmed persistent perforation.
Patient was deemed to be a very high-risk surgical candidate for mortality due to worsening comorbidities including cirrhosis secondary to MASH, and development of hepatorenal syndrome requiring dialysis. MELD Na score had worsened to 43 points (90-day mortality risk of 95.9%). Mayo clinic post-operative mortality risk in patients with cirrhosis was also calculated to be 94.3% at 7 days interval. Goals of care were discussed and the decision was made to attempt endoscopic repair because the patient had high surgical risk for mortality.
Endoscopic repair was performed by application of Argon Plasma Coagulation (APC) ablation followed by clip closure (Mantis Clip x 2- Boston Scientific, Lockado 16mm clip x 4-Microtech). Successful repair was confirmed fluoroscopically. A repeat upper GI series was performed which confirmed successful repair of gastric antral leak and diet was resumed. Discussion: This case highlighted the importance of providing appropriate, minimally invasive, and timely interventions. Peptic ulcers carry a significant risk of mortality when not managed effectively. This presented a unique opportunity to explore an alternative approach as the patient was a very high-risk surgical candidate. Endoscopic intervention spared him the additional risks associated with another surgery, improving patient outcomes. Compiling additional data on this technique may help determine whether it offers significant advantages over traditional surgical re-exploration, potentially shaping future clinical guidelines.
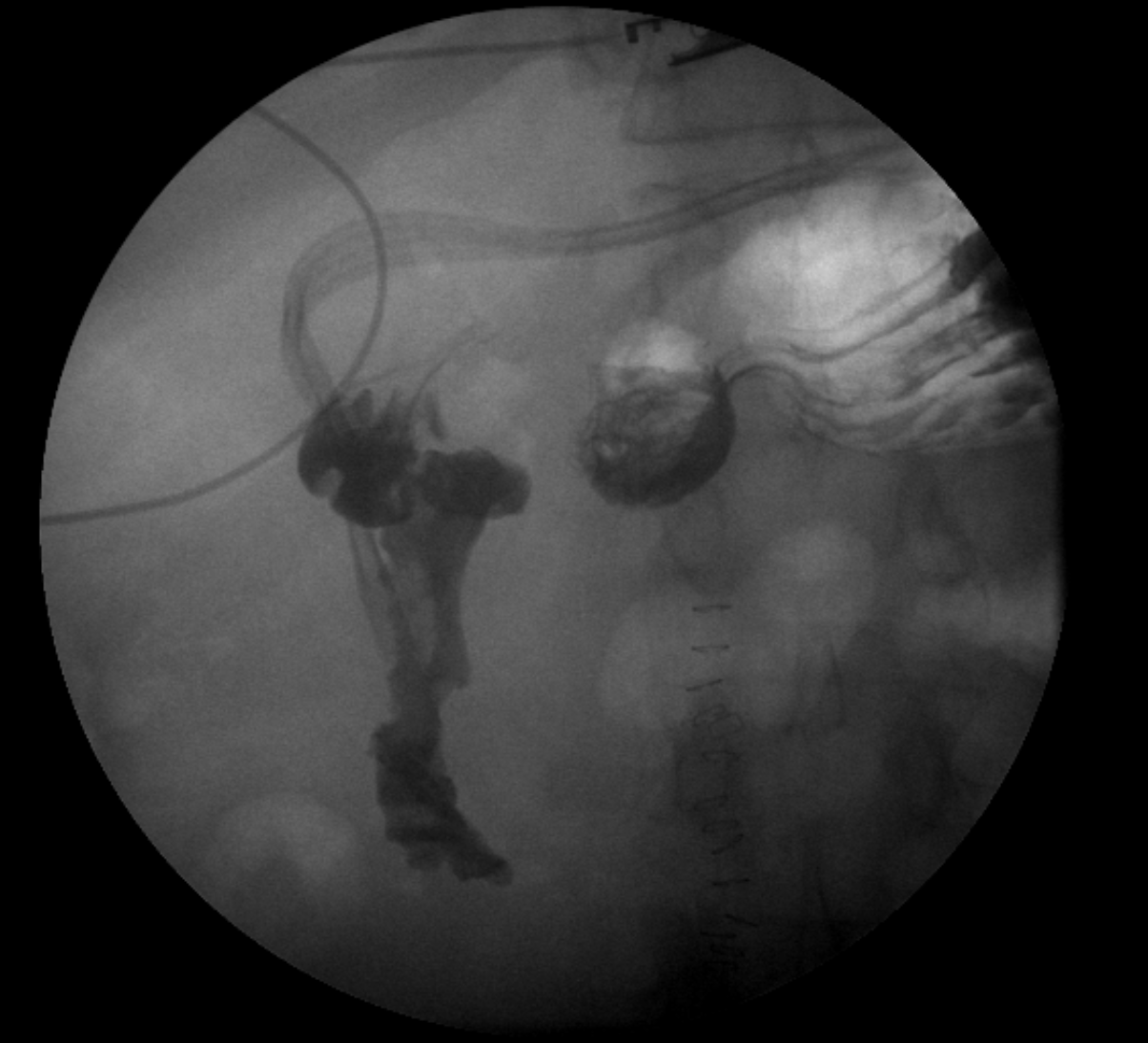
Figure: Persistent Leak after Graham Patch Repair on GI series confirmed
Figure: Successful Post-Endoscopic Repair on GI series confirmed
Disclosures: Usman Rahim indicated no relevant financial relationships. Bukhtawar Munir indicated no relevant financial relationships. Dragos Pausescu indicated no relevant financial relationships. Johnson Yeboah indicated no relevant financial relationships.
Usman Rahim, MD1, Bukhtawar Munir, MD2, Dragos Pausescu, MD2, Johnson Yeboah, MD3. P5718 - Endoscopic Closure of Gastric Perforation in a Patient With Liver Failure, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")