Creighton University School of Medicine Phoenix, AZ
Award: ACG Presidential Poster Award
Vishnu Yanamaladoddi, MD1, Vikash Kumar, MD1, Shree Laya Vemula, MD2, Sandeep Chikkam, MD, DNBSS3, Pir Shah, MD1, Indu Srinivasan, MD1 1Creighton University School of Medicine, Phoenix, AZ; 2NYC Health + Hospitals/South Brooklyn Health, Brooklyn, NY; 3Asian Institute of Gastroenterology, Hyderabad, Telangana, India Introduction: Duodenal ulcers are surgical emergencies often managed with a Graham patch repair. Persistent leaks may occur, sometimes progressing to entero-cutaneous fistulas. Traditionally, these complications are treated with surgical re-patching or gastrojejunostomy to divert enteric contents and promote healing. Lumen-apposing metal stents (LAMS), originally designed to create secure fistulous tracts, have seen expanded clinical use. We present the case of a 70-year-old who developed a duodenal-cutaneous fistula following Graham patch repair and was successfully treated with a LAMS.
Case Description/
Methods: A 70-year-old female with type 2 diabetes and complex surgical history including Graham patch repair of a perforated duodenal ulcer and open cholecystectomy presented with two weeks of right upper quadrant pain, erythema over a surgical scar, and fever. She had chronic postoperative drainage and recurrent abscesses for two years. Imaging revealed a 6.5 cm gas and fluid collection with a fistulous tract from the duodenal bulb to a collection in the gallbladder fossa extending into the abdominal wall, consistent with an enteric-origin abscess. Initial management included bedside incision and drainage with empiric antibiotics. Endoscopy identified a duodenal ulcer with an embedded suture but no active bleeding or visible fistula. A percutaneous drain was placed for abdominal abscess drainage, and the suture was removed endoscopically using a loop cutter and Roth forceps. To promote healing, a LAMS was placed endoscopically from the pylorus to the second portion of the duodenum, bypassing the affected area. The patient’s symptoms improved, and follow-up CT with oral contrast showed no leakage. On serial follow-up, the cutaneous wound healed completely. After elective LAMS removal, a duodenal stricture was noted and dilated. The patient reported complete resolution of her symptoms. Discussion: Endoscopic creation of a stomach-to-small bowel bypass using LAMS represents a groundbreaking advancement in managing complex duodenal ulcer complications. This minimally invasive approach offers a promising alternative for persistent duodenal leaks or fistulas, especially after Graham patch failure where surgical options carry significant risk. Early reports demonstrate high technical success with ulcer healing and fistula closure, avoiding invasive reoperation. While this approach shows remarkable promise, long-term data is needed to validate durability and safety.
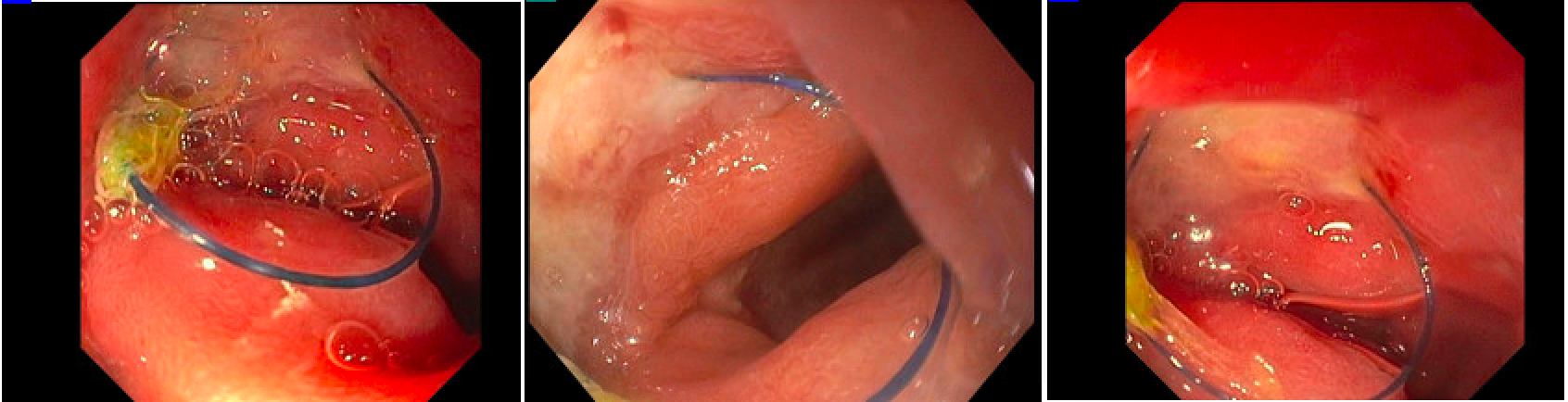
Figure: 1 - Persistent duodenal suture from Graham patch repair