P5711 - Palliating the Unpalliable: EUS-Guided Gastrojejunostomy Using AXIOS Stent for Malignant Small Bowel Obstruction in Advanced Rectal Adenocarcinoma
Mohamed Belal, MD1, Rutwik Pradeep. Sharma, MD2, Abhishek Satishchandran, MD, PhD3 1McLaren Flint Hospital, Grand Blanc, MI; 2University of Michigan-Sparrow Hospital, Lansing, MI; 3University of Michigan, Lansing, MI Introduction: Malignant small bowel obstruction due to peritoneal carcinomatosis presents a therapeutic challenge particularly in patients deemed inoperable. Endoscopic ultrasound-guided gastrojejunostomy (EUS-GJ) with lumen-apposing metal stents (LAMS) has emerged as a minimally invasive alternative to surgery. We present a 52-year-old female with KRAS G12D-mutant rectal adenocarcinoma metastatic to liver, lung, and peritoneum, complicated by closed-loop SBO. Deemed inoperable due to carcinomatosis and poor nutrition, she underwent EUS-GJ with a 15x10 mm AXIOS stent, resulting in immediate drainage of enteric contents and rapid decompression. Serial CT scans confirmed successful bypass of the obstruction, with marked improvement in small bowel distention. She experienced rapid symptom relief and resumed oral intake, transitioning to hospice care.
Case Description/
Methods: A 52-year-old female with KRAS G12D-mutant rectal adenocarcinoma metastatic to liver, lung, and peritoneum, previously treated with chemotherapy, presented with worsening abdominal pain, distention, and gastrostomy tube cessation. CT Abdomen/Pelvis showed closed-loop SBO. Surgery deemed her inoperable due to carcinomatosis and poor nutrition. After multidisciplinary discussion, EUS-guided gastrojejunostomy was performed, deploying a 15x10 mm AXIOS stent between the gastric body and jejunum. The stent was dilated, anchored with double pigtail stents, and enteric contents drained immediately.
Traditional management options, including surgical gastrojejunostomy or enteral stenting, are often limited by high morbidity or risk of recurrent obstruction. EUS-GJ creates an internal bypass while minimizing procedural risks, offering rapid symptom relief and improved quality of life. Recent studies (Tyberg et al.) report 92% technical and 85% clinical success rates with EUS-GJ, with low adverse event rates. Additional reports (Mba Eya et al., Westerveld et al., Mitsuhashi et al.) demonstrate innovative applications of LAMS for malignant bowel obstructions, including colonic-enteric and ileosigmoidostomy anastomoses.
Discussion: Our case contributes to this growing evidence by illustrating the clinical, radiologic, and palliative benefits of EUS-GJ in malignant SBO secondary to peritoneal carcinomatosis. The patient’s course exemplifies how EUS-GJ can provide a viable, minimally invasive palliative option for inoperable patients. Further studies are needed to standardize protocols and refine patient selection to maximize benefits.
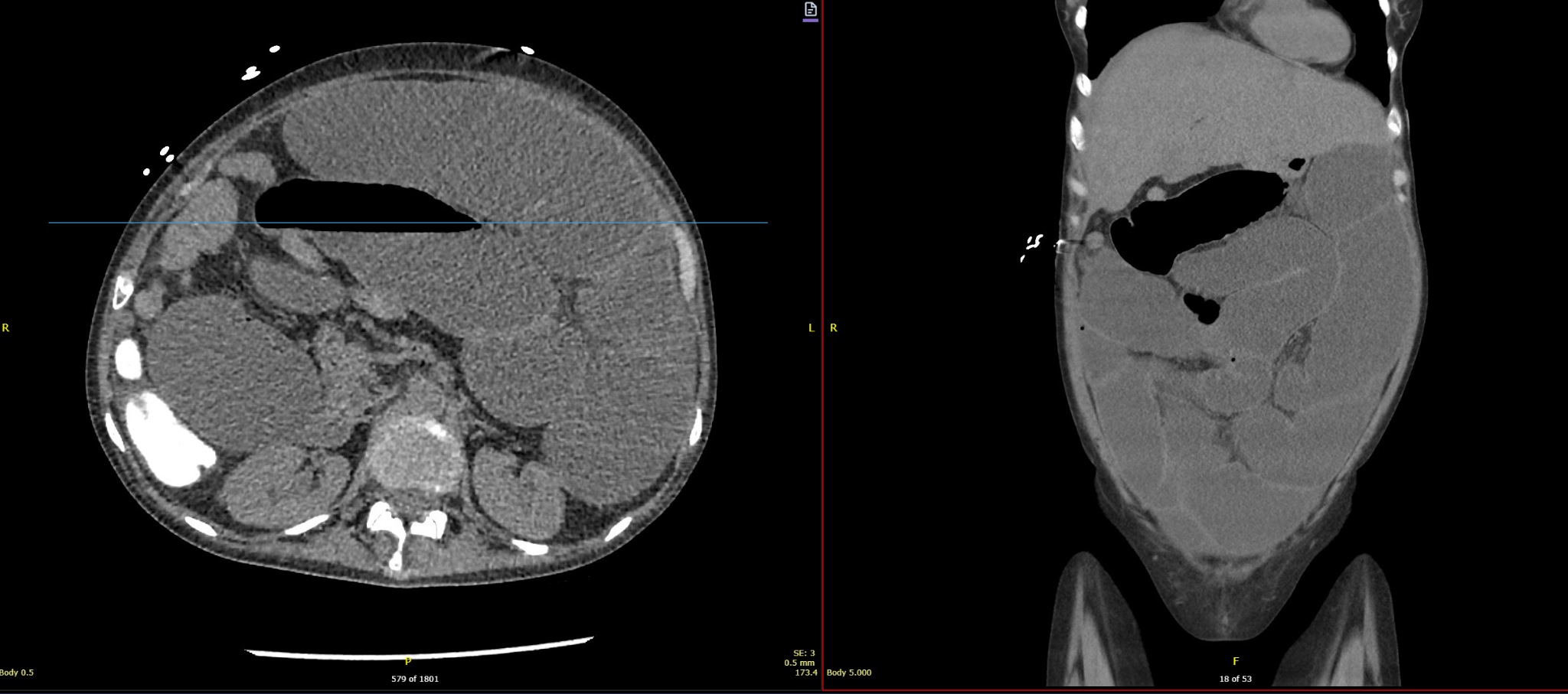
Figure: CT abdomen pelvis without IV contrast 4/25/25 axial(left) and coronal(right side) section- SBO- dilated small bowel loops with air fluid levels.
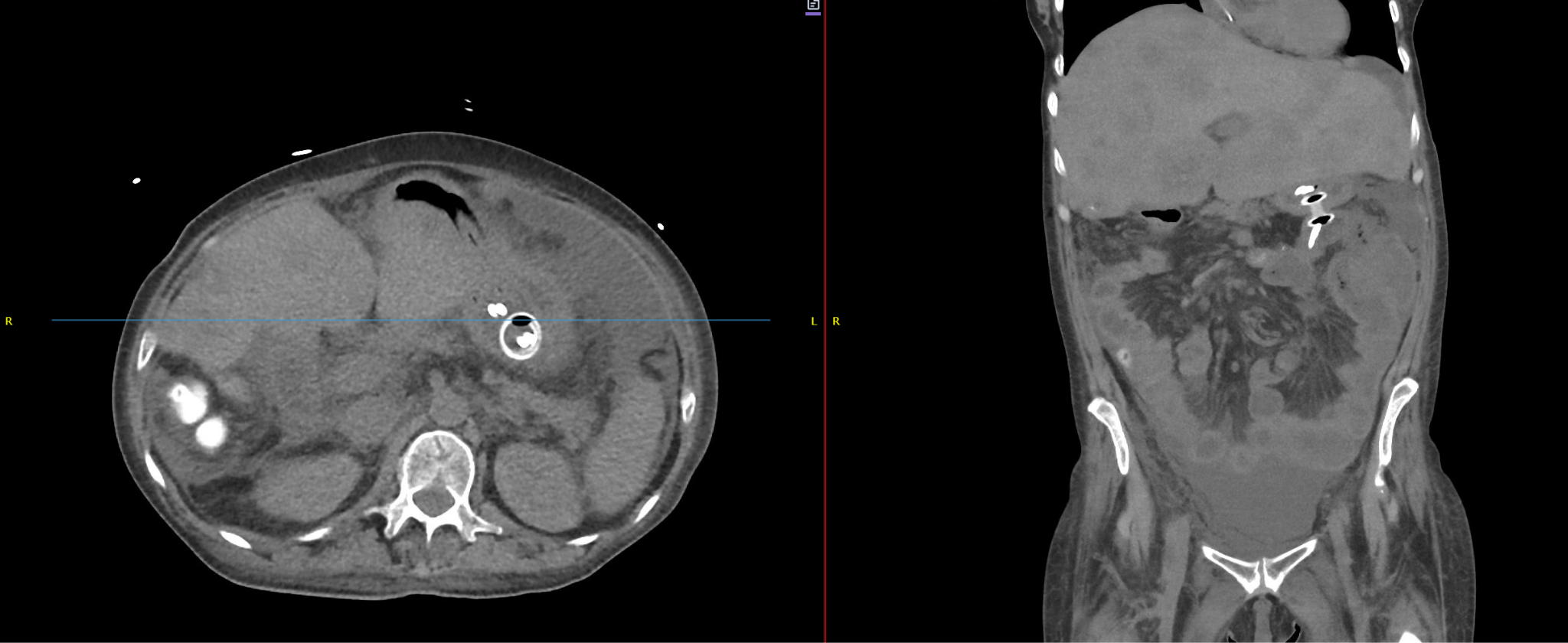
Figure: CT abdomen pelvis without IV contrast 4/28/25 axial(left) and coronal(right side) section- status post gastrojejunal lumen opposing metal stent placement with resolution of small bowel obstruction.
Disclosures: Mohamed Belal indicated no relevant financial relationships. Rutwik Sharma indicated no relevant financial relationships. Abhishek Satishchandran indicated no relevant financial relationships.
Mohamed Belal, MD1, Rutwik Pradeep. Sharma, MD2, Abhishek Satishchandran, MD, PhD3. P5711 - Palliating the Unpalliable: EUS-Guided Gastrojejunostomy Using AXIOS Stent for Malignant Small Bowel Obstruction in Advanced Rectal Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.