Robert Krahmer, MD1, Joseph Moore, MD1, Jonathan Hilal, MD2 1University of South Florida, Tampa, FL; 2Tampa General Hospital / University of South Florida, Tampa, FL Introduction: Endoscopic retrograde cholangiopancreatography (ERCP) is a common procedure for the treatment of pancreaticobiliary disorders. While ERCP is considered a safe procedure, there are several well-described complications including pancreatitis, intestinal perforation, and intraluminal bleeding. Splenic injury is a rare, but potentially fatal complication that must be quickly recognized by the endoscopist.
Case Description/
Methods: A 71-year-old female with no past medical history underwent endoscopic ultrasound with biopsy and ERCP with biliary stent placement for a pancreatic head mass. The ERCP was technically challenging due edema and extrinsic compression of the duodenum, necessitating a long scope position to locate the major papilla. Numerous attempts were made to access the bile duct including double wire technique after the ventral pancreatic duct was inadvertently cannulated, but biliary cannulation was ultimately unsuccessful. The following day, she developed epigastric pain, vomiting, and lethargy. Vitals showed the patient to be hypothermic (94.5 °F) and hypotensive (89/52). Labs were notable for an acute attenuation in hemoglobin to 7.5 g/dL from 10.8 g/dL preoperatively, leukocytosis of 13.02 cells/mL, and lactic acidosis of 5.5 mg/dL. She was transferred to the ICU and started on vasopressors. A STAT CT angiogram of the abdomen demonstrated a high-grade splenic injury with moderate volume hemoperitoneum and active contrast extravasation extending into the left posterior peritoneum. She was taken for emergent embolization with interventional radiology and coil embolization of the proximal splenic artery was performed. She stabilized following embolization and was eventually able to be safely discharged. Discussion: Splenic injury is a rare but serious complication of ERCP. Our literature review found 37 documented cases of ERCP-related splenic injury. It is hypothesized these injuries are due to forces applied to the greater curvature of the stomach by the endoscope which are transmitted to the spleen via the gastrosplenic ligament. These forces are greatest when the endoscope is in the long position. Therefore, it is reasonable to speculate that technically challenging ERCPs, particularly cases requiring prolonged use of the long position, have the most risk of splenic injury. Treatment of ERCP-related splenic injury is usually splenectomy. However, our patient did well with splenic artery embolization and splenectomy was not required.
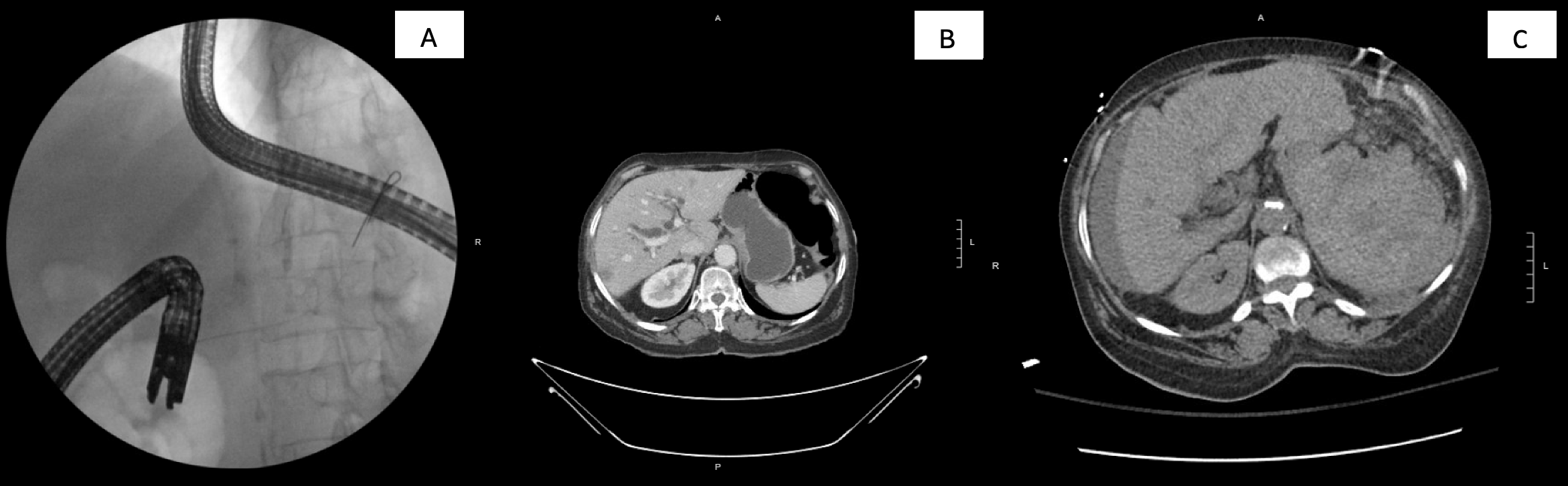
Figure: A. Duodenoscope in the long-scope position with a guidewire in the pancreatic duct. B. Normal spleen from 1 week prior to ERCP. C. Grade 4/5 splenic laceration with hemoperitoneum.
Disclosures: Robert Krahmer indicated no relevant financial relationships. Joseph Moore indicated no relevant financial relationships. Jonathan Hilal indicated no relevant financial relationships.
Robert Krahmer, MD1, Joseph Moore, MD1, Jonathan Hilal, MD2. P5706 - A Rare Complication of Post-ERCP Splenic Injury, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.