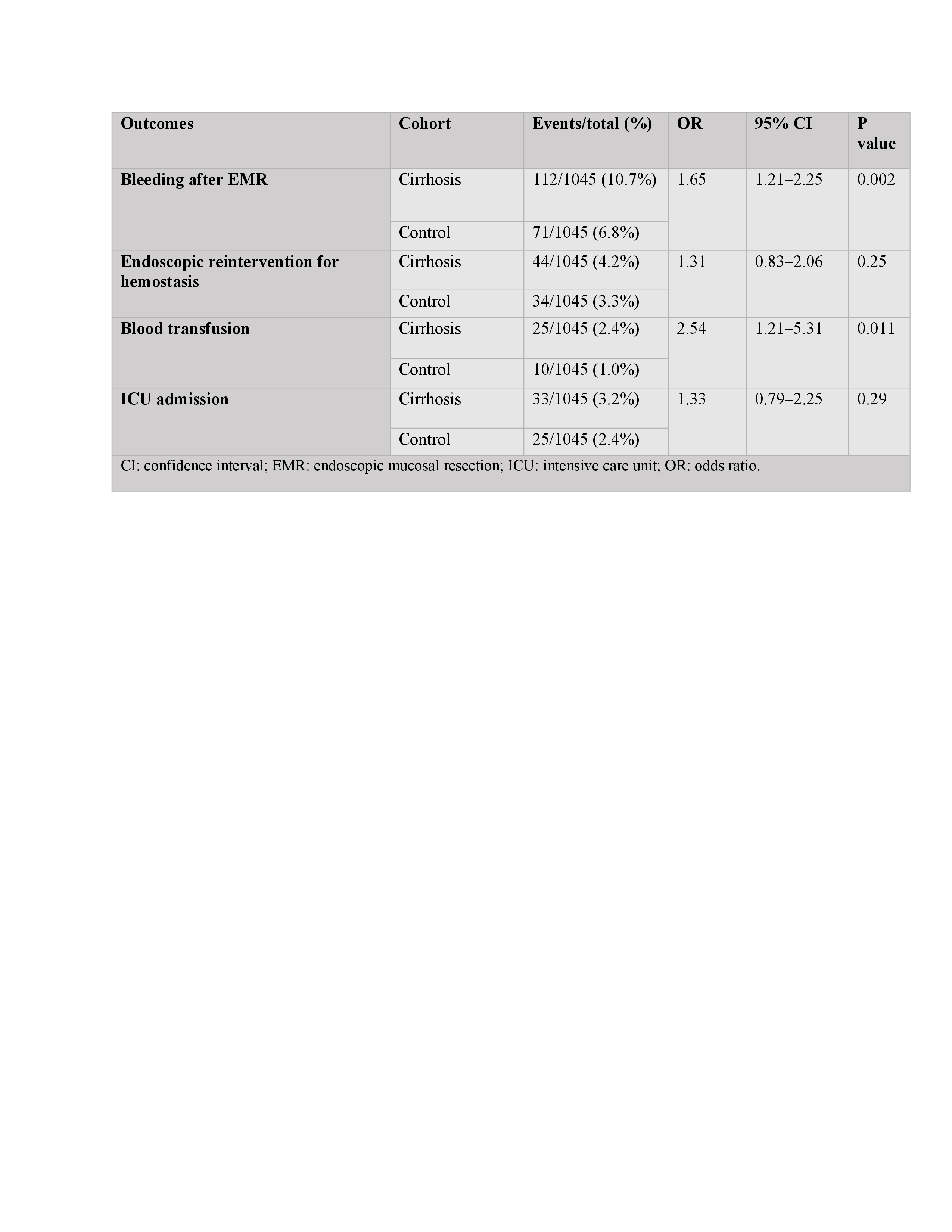
Razan Aburumman, MD1, Saqr Alsakarneh, MD, MSc2, Sumit Singla, MD1 1Henry Ford Health, Detroit, MI; 2Mayo Clinic, Rochester, MN Introduction: Esophagogastroduodenoscopy (EGD) with endoscopic mucosal resection (EMR) is a procedure used for evaluation and management of different upper gastrointestinal lesions. However, cirrhosis-associated coagulopathy and portal hypertension may increase the risk of post-procedural complications. This study aimed to evaluate the 30-day risk of bleeding and other adverse outcomes following EGD with EMR in patients with cirrhosis compared to matched non-cirrhotic controls. Methods: This retrospective cohort study utilized data from the US Collaborative Network to evaluate the risk of bleeding following Esophagogastroduodenoscopy with EMR in patients with cirrhosis compared to matched controls. One-to-one propensity score matching was employed, with the primary outcome being bleeding within 30 days of the procedure. Bleeding risk was further analyzed based on cirrhosis severity, categorized as compensated or decompensated. Results: After propensity score matching, each cohort included 1,045 patients. Patients with cirrhosis had a higher risk of post-EMR bleeding (OR 1.65, 95% CI 1.21–2.25, P = 0.002) and were more likely to require blood transfusion (OR 2.54, 95% CI 1.21–5.31, P = 0.011). However, ICU admissions (OR 1.33, 95% CI 0.79–2.25, P = 0.29) and endoscopic reinterventions (OR 1.31, 95% CI 0.83–2.06, P = 0.25) were not significantly different between cohorts.
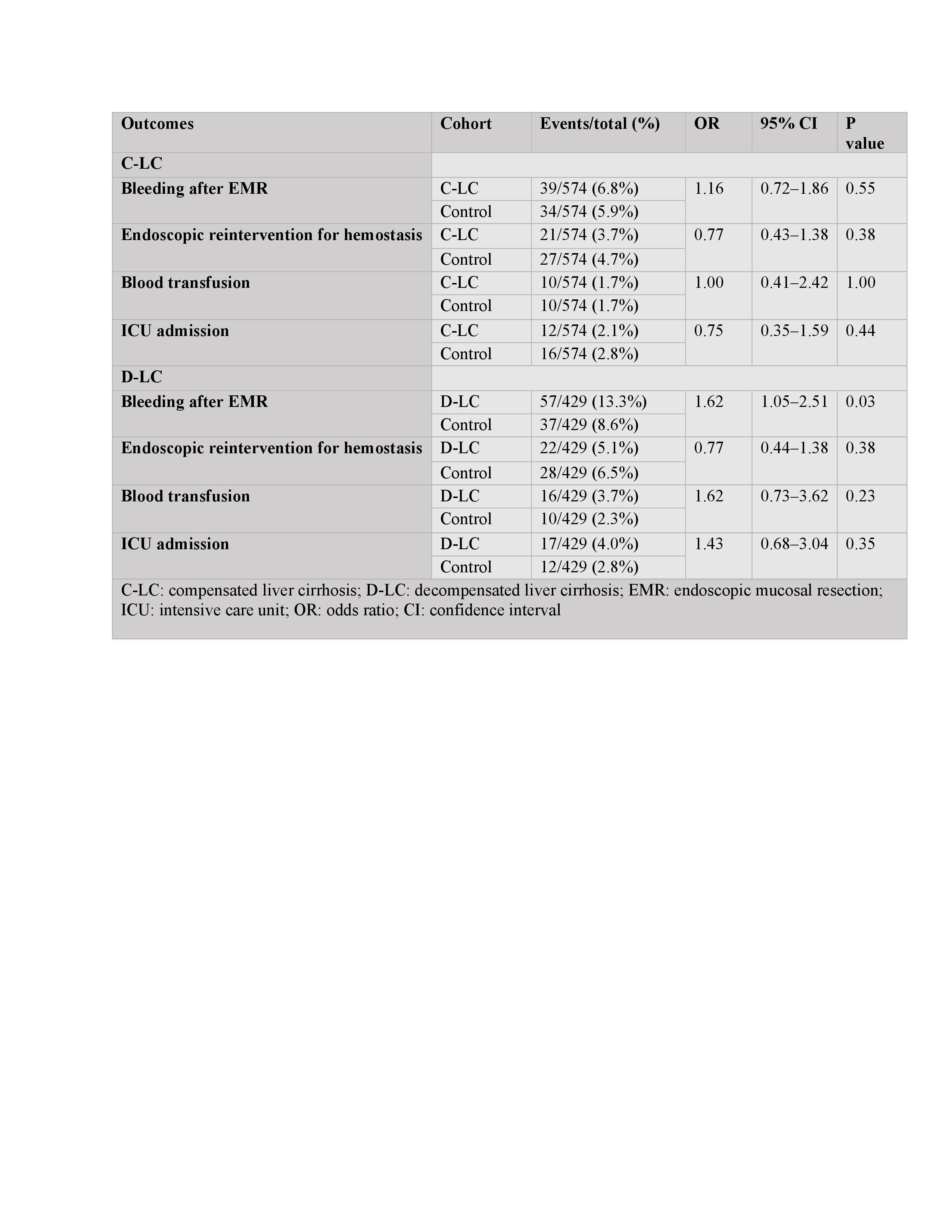
Patients with decompensated cirrhosis had a significantly higher risk of post-EMR bleeding compared to controls (OR 1.62, 95% CI 1.05–2.51, P = 0.03), whereas patients with compensated cirrhosis did not demonstrate an increased bleeding risk (OR 1.16, 95% CI 0.72–1.86, P = 0.55). Additionally, ICU admission, blood transfusion, and reintervention rates were not significantly different from controls in either group. Discussion: This matched cohort study found increased rates of post-procedural bleeding and transfusion in cirrhotic patients undergoing EGD with EMR, primarily among those with decompensated disease. Compensated cirrhosis was not associated with higher complication rates. These results highlight the importance of optimizing coagulopathy and carefully planning the procedure in patients with decompensated cirrhosis.
Figure: Table 1: Clinical outcomes within 30 days of EMR in cirrhosis compared with the matched control group
Figure: Table 2: Clinical outcomes within 30 days of EMR in compensated and decompensated liver cirrhosis compared with the matched control group
Disclosures: Razan Aburumman indicated no relevant financial relationships. Saqr Alsakarneh indicated no relevant financial relationships. Sumit Singla: Boston Scientific. – Consultant.
Razan Aburumman, MD1, Saqr Alsakarneh, MD, MSc2, Sumit Singla, MD1. P5697 - Risk of Bleeding After Esophagogastroduodenoscopy With Mucosal Resection in Patients With Cirrhosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.