Rahul Borra, DO, Tong Ren, MD, Salman Muddassir, MD, Guesly Delva, MD HCA Healthcare, Brooksville, FL Introduction: Pylephlebitis is a rare suppurative infection of the portal venous system that carries significant morbidity and mortality. Here we present a case of pylephlebitis in a patient who presented with abdominal pain and fever.
Case Description/
Methods: 56 year-old male with a history of end-stage liver disease due to untreated hepatitis C, portal hypertension and recurrent ascites presented with 2 week history of worsening abdominal pain and subjective fevers. Pain was worst in the right upper quadrant, described as aching, rated a 8/10 in severity, with no aggravating or relieving factors. Patient was hypertensive and tachycardic on arrival. CBC showed WBC 5.6, hemoglobin 6.9, with MCV 67.1. LFTs showed AST 72, ALT 54, alkaline phosphatase 78, and total bilirubin at 1.7. Ammonia was 40. Abdomen was severely distended on physical exam. CT abdomen/pelvis revealed a cirrhotic liver with a large thrombus in the main portal vein with extension in the right portal vein, splenomegaly and extensive collateral vessels in the upper abdomen and lower esophagus. Blood cultures were collected and the patient was started on diuretics, albumin, and lactulose. Ceftriaxone was started due to concern for SBP. Paracentesis removed 6.7 L of fluid and analysis was negative for any infection. Gastroenterology, Infectious Disease and Hematology were consulted. Due to concern for bleeding, GI performed EGD, which revealed grade 3 esophageal varices that were banded. Per Hematology, unfractionated heparin was started, however soon stopped due to lower extremity bleeding. Cultures returned positive for Streptococcus group G. Due to bacteremia with a known thrombus in the portal vein system, patient was diagnosed with pylephlebitis. ID recommended 6 weeks of IV Rocephin. With antibiotic administration, the patient symptomatically improved, and he was discharged home with a referral for a liver transplant.
Discussion: Pylephlebitis, or septic portal vein thrombosis, should be considered in individual who present with fever and abdominal pain and have evidence of thrombosis on imaging studies. The most common etiologies are intra-abdominal infections that spread to the portal venous system. A diagnostic challenge due to the overlying co-morbidities that individual with this condition typically have, the disease carries significant morbidity and mortality and should not be missed. If diagnosed, IV antibiotics are mainstay treatment, while the use of concurrent anticoagulation is still hotly debated.
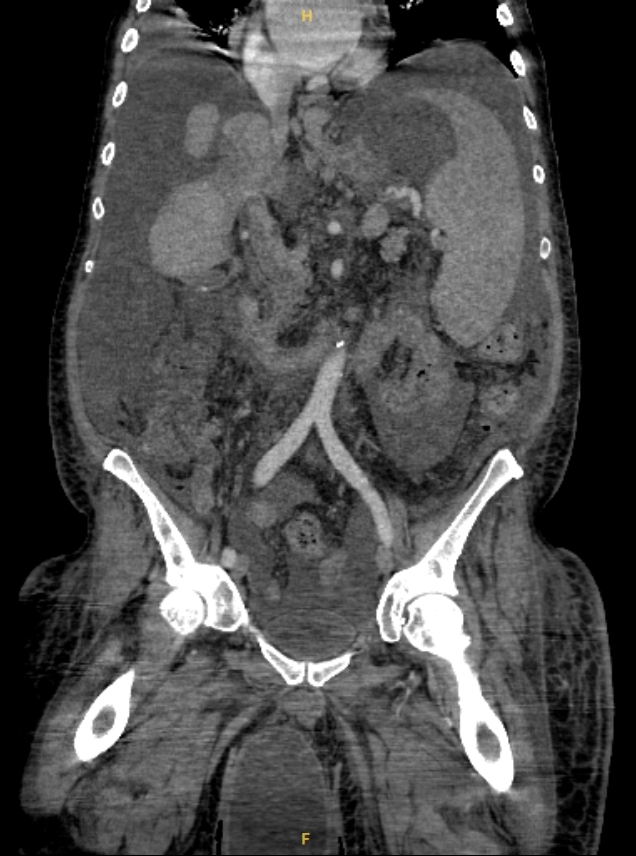
Figure: Coronal view of CT Abdomen/Pelvis which demonstrates portal vein thrombus
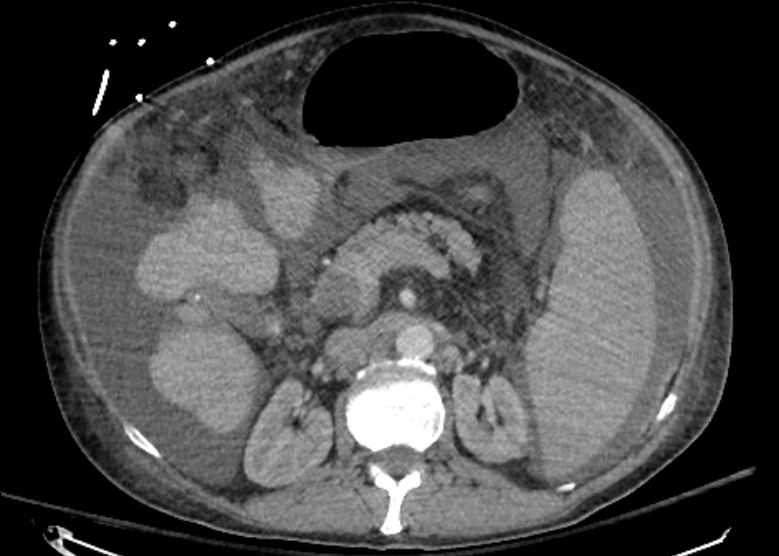
Figure: Axial view of CT Abdomen/Pelvis which demonstrates thrombus in the portal vein in addition to extensive abdominal ascites
Disclosures: Rahul Borra indicated no relevant financial relationships. Tong Ren indicated no relevant financial relationships. Salman Muddassir indicated no relevant financial relationships. Guesly Delva indicated no relevant financial relationships.
Rahul Borra, DO, Tong Ren, MD, Salman Muddassir, MD, Guesly Delva, MD. P5625 - An Uncommon Culprit in Common Symptoms: A Case of Pylephlebitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")