Creighton University School of Medicine Phoenix, AZ
Award: ACG Presidential Poster Award
Vishnu Yanamaladoddi, MD1, Ariana R. Tagliaferri, MD1, Shree Laya Vemula, MD2, Amla Patel, MBBS3, John Brown, MD1, Danlu Wang, DO1 1Creighton University School of Medicine, Phoenix, AZ; 2NYC Health + Hospitals/South Brooklyn Health, Brooklyn, NY; 3Creighton University, Phoenix, Phoenix, AZ Introduction: Coccidioidomycosis is a fungal infection endemic to desert regions such as the southwestern United States. Most infected patients are asymptomatic or have respiratory symptoms. Dissemination occurs in < 1% of cases. Common sites include skin, joints, and CNS, while peritoneal and omental involvement is extremely rare. Hematogenous spread from pulmonary infection is most common, though direct seeding via infected sputum is possible. We describe a case of a young male presenting with eosinophilia and ascites, ultimately diagnosed with omental coccidioidomycosis.
Case Description/
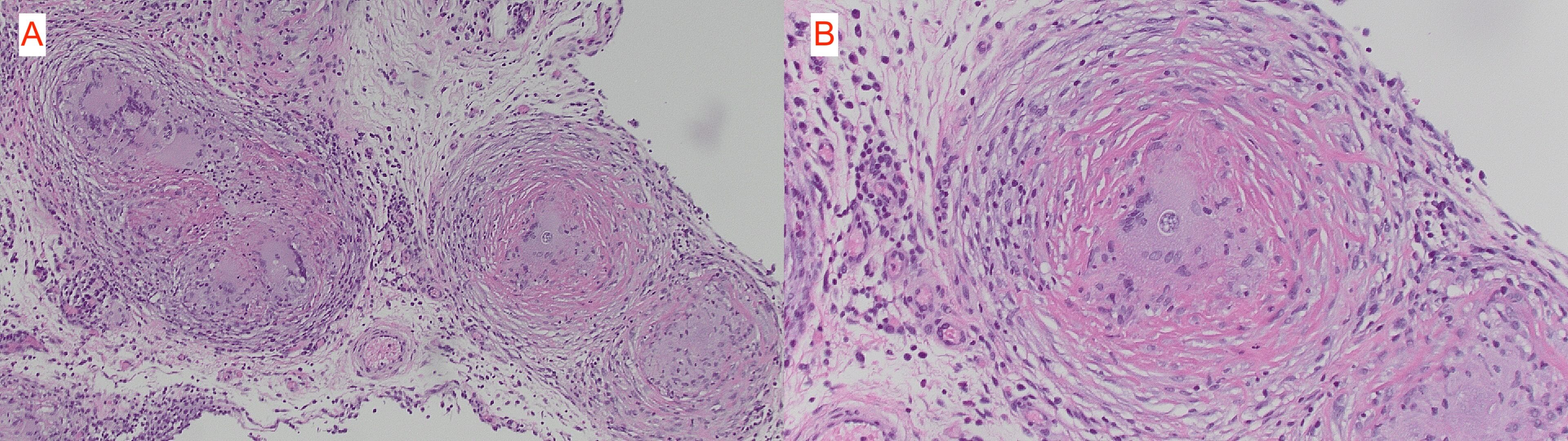
Methods: A 31-year-old Haitian man, who immigrated 6 months prior, presented with progressive abdominal pain and distention for three weeks. He denied fevers, night sweats, weight loss, or respiratory symptoms. He was afebrile, hemodynamically stable, and had ascites without other stigmata of chronic liver disease. Labs were notable for eosinophilia (14.9%, absolute 800/uL); liver function and albumin (4 g/dL) were normal. CT showed large ascites, omental nodularity, mesenteric inflammation with lymphadenopathy, and a right lower lobe pulmonary nodule. Paracentesis revealed inflammatory ascitic fluid (WBC 5859/mm³) with eosinophils and histiocytes; cytology and cultures were negative. Extensive infectious, autoimmune, parasitic workup, and endoscopy with biopsies were unrevealing. Though coccidioides IgG and CF titer were positive (1:64), peritoneal cocci serologies were negative. Due to refractory ascites, exploratory laparotomy revealed miliary omental and peritoneal nodules. Biopsies showed non-necrotizing granulomas with fungal spherules consistent with Coccidioides immitis. He was discharged on high-dose fluconazole and at 6 weeks follow up his ascites resolved and did not recur. Discussion: This case highlights an extremely rare presentation of disseminated coccidioidomycosis with omental involvement manifesting as eosinophilic ascites. Diagnosis was delayed due to absent respiratory symptoms and negative peritoneal studies. Omental biopsy ultimately unveiled the diagnosis. Clinicians should maintain high suspicion for disseminated coccidioidomycosis in endemic areas and unexplained eosinophilia. Early recognition and antifungal therapy can result in full clinical resolution.
Disclosures: Vishnu Yanamaladoddi indicated no relevant financial relationships. Ariana Tagliaferri indicated no relevant financial relationships. Shree Laya Vemula indicated no relevant financial relationships. Amla Patel indicated no relevant financial relationships. John Brown indicated no relevant financial relationships. Danlu Wang indicated no relevant financial relationships.
Vishnu Yanamaladoddi, MD1, Ariana R. Tagliaferri, MD1, Shree Laya Vemula, MD2, Amla Patel, MBBS3, John Brown, MD1, Danlu Wang, DO1. P5618 - Unmasking Eosinophilic Ascites: A Rare Case of Omental Coccidioidomycosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.