P5600 - Concurrent Herpes Simplex Virus Esophagitis and Cytomegalovirus Gastritis in an Immunocompromised Patient with Metastatic Endometrial Carcinoma and Immune Checkpoint Inhibitor Hepatitis
Yale New Haven Health, Bridgeport Hospital Bridgeport, CT
Prince A. Ameyaw, MD1, Ujunwa Korie, MD, MS2, George M. Hanna, MD1 1Yale New Haven Health, Bridgeport Hospital, Bridgeport, CT; 2Yale New Haven Hospital, New Haven, CT Introduction: Herpes simplex virus (HSV) and Cytomegalovirus (CMV) are common causes of gastrointestinal opportunistic infections in immunocompromised hosts. However, regardless of the degree or type of immunosuppression, coexisting opportunistic viral infections in the gastrointestinal tract remain rare. We present a case of concurrent HSV esophagitis and CMV gastritis in an immunocompromised patient.
Case Description/
Methods: A 67-year-old female with metastatic endometrial carcinoma status post-surgical resection on adjuvant chemotherapy and immunotherapy complicated by immune checkpoint inhibitor (ICI) hepatitis treated with high-dose prednisone presented with recurrent abdominal pain worse in the right upper quadrant (RUQ) and exacerbated by eating. She denied fever, melena, dysphagia, or odynophagia. The physical examination was remarkable for RUQ and epigastric tenderness with a negative Murphy sign. Labs showed elevated WBC 14.4 and ANC 13,200 , low absolute lymphocyte count 270 and an increase in her liver enzymes, reflecting her ICI-hepatitis. An abdominal ultrasound showed cholelithiasis, no portal vein thrombosis, and was otherwise normal. Intravenous pantoprazole was started. Endoscopic ultrasound was negative for obstructing stones or pancreaticobiliary dilatation, but it revealed pan-esophageal white nummular lesions and three non-bleeding gastric ulcers without stigmata of bleeding. Histopathology revealed esophageal squamous cells with HSV inclusions (figure 1) and ulcerated gastric antral mucosa with CMV inclusions (figure 2), consistent with herpetic esophagitis and CMV gastritis. Additional fungal stains were negative. Valganciclovir was initiated for 21 days, leading to the resolution of abdominal pain. However, the patient continued to experience worsening liver enzyme elevations and was started on ursodiol, fenofibrate, and mycophenolate mofetil alongside a tapering steroid course with a favorable response. Discussion: The morbidity of HSV and CMV gastrointestinal infections is determined by the host immune response. The increasing utilization of ICI immunotherapy in cancer treatment has been associated with a parallel increase in immune-related adverse events (irAEs). Corticosteroid therapy for irAEs in cancer patients risks further worsening the severity of immunosuppression and predisposes patients to opportunistic infections. A high index of suspicion for concurrent gastrointestinal opportunistic infections is required in immunocompromised patients to reduce morbidity.
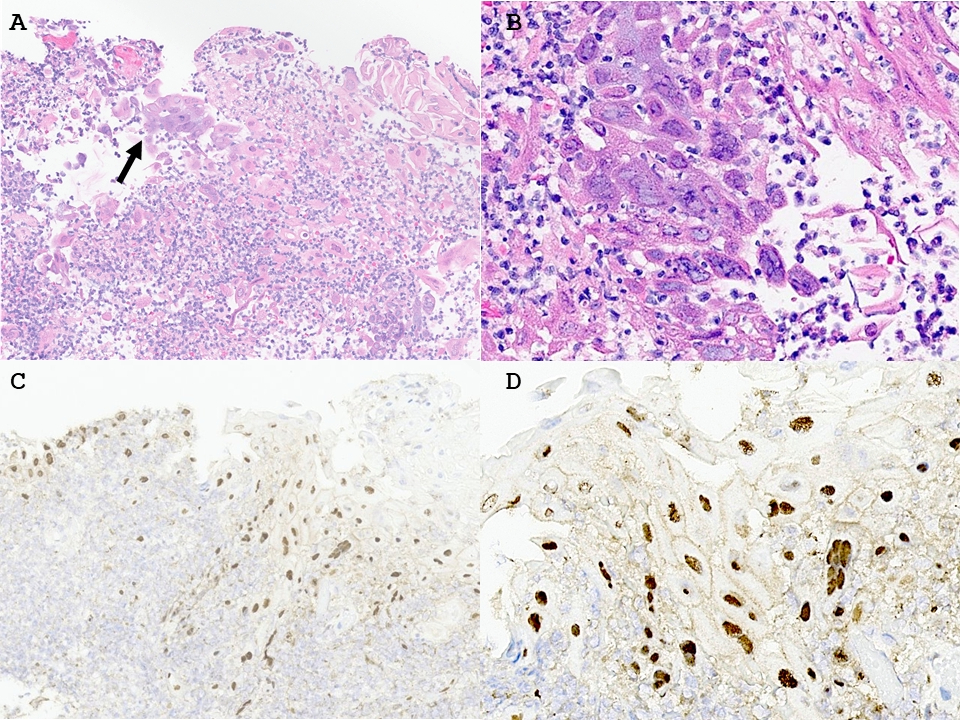
Figure: Figure 1: HSV esophagitis. (A) A medium power view of the esophageal biopsy shows fibrinopurulent debris and sloughed squamous epithelial cells. A cluster of squamous cells shows glassy nuclear changes consistent with herpetic viral cytopathic effect (arrow). (B) High-power view of the area indicated by the arrow in figure 1A shows squamous cells with classic HSV cytopathic changes characterized by multinucleation, nuclear molding and peripheral chromatin margination with a ground glass appearance. (C) An immunohistochemical stain for HSV confirms the presence of HSV in many squamous epithelial cells. (D) An immunohistochemical stain for HSV shows strong nuclear positivity in the epithelial cells with HSV viral cytopathic changes, confirming the diagnosis of HSV esophagitis
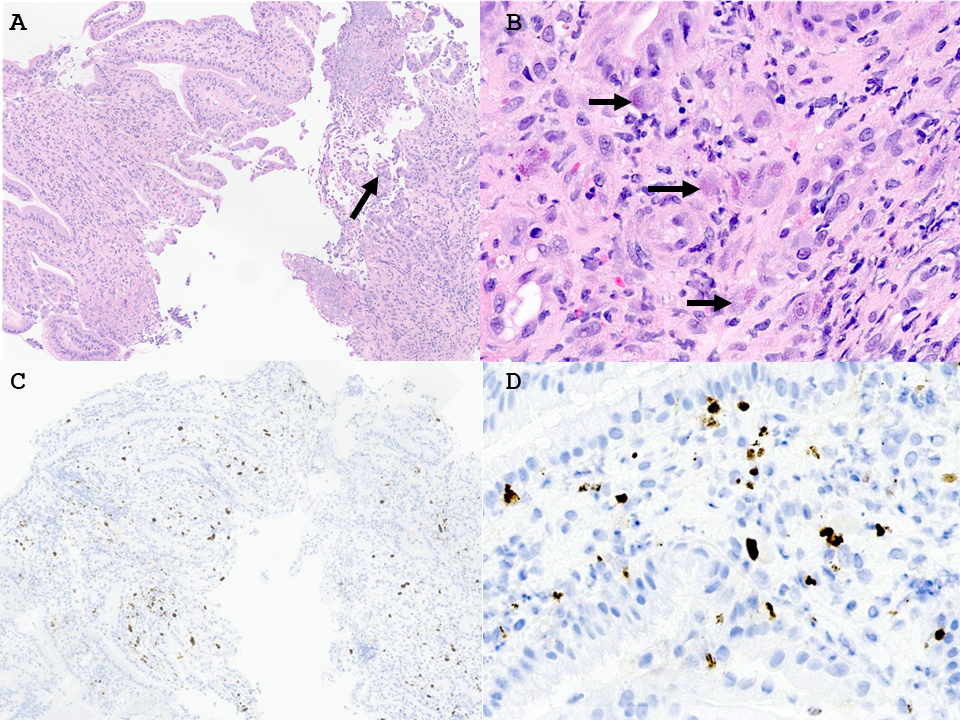
Figure: Figure 2: CMV gastritis. (A) A medium-power view of the stomach biopsy shows ulcerated gastric mucosa with inflammation and fibrinopurulent debris (arrow). (B) High-power image of the stroma of the gastric biopsy demonstrates scattered enlarged (cytomegalic) cells with enlarged glassy eosinophilic nuclear inclusions and eosinophilic granular cytoplasmic inclusions characteristic of CMV. (C) An immunohistochemical stain for CMV highlights numerous CMV viral inclusions scattered within the gastric biopsy. (D) An immunohistochemical stain for CMV highlights numerous CMV viral inclusions in the gastric biopsy stroma.
Disclosures: Prince Ameyaw indicated no relevant financial relationships. Ujunwa Korie indicated no relevant financial relationships. George Hanna indicated no relevant financial relationships.
Prince A. Ameyaw, MD1, Ujunwa Korie, MD, MS2, George M. Hanna, MD1. P5600 - Concurrent Herpes Simplex Virus Esophagitis and Cytomegalovirus Gastritis in an Immunocompromised Patient with Metastatic Endometrial Carcinoma and Immune Checkpoint Inhibitor Hepatitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")