Maher Taha, MD1, Lana Dardari, MD2, Arthur CHIDI. Igbo, MD, MPH3, Amna Naveed Butt, MD4, Angelin Raju, MD5 1Texas Health Resources, Irving, TX; 2Cleveland Clinic Foundation, Westlake, OH; 3Texas Health Resources HEB/Denton Internal Medicine Program, Lewisville, TX; 4Texas Health Resources, Haslet, TX; 5Texas Health Resources HEB/ Denton, Bedford, TX Introduction: Inflammatory bowel disease (IBD) encompasses a group of gastrointestinal disorders, including Crohn’s disease and ulcerative colitis. These conditions present with diarrhea, abdominal discomfort, and hematochezia, which can be seen in a variety of infectious or inflammatory processes. Yersinia enterocolitica is a gram-negative bacterium that can lead to mucosal inflammation and ulceration, which can closely resemble IBD clinically and endoscopically. Diagnosing IBD prematurely can lead to inappropriate treatment and adverse outcomes.
Case Description/
Methods: An 87-year-old woman with a history of hypertension and GERD presented with multiple episodes of bloody stools. She had a similar episode four months prior, where flexible sigmoidoscopy showed findings suggestive of early IBD. Infectious workup at the time was negative, but she was lost to GI follow-up. Colonoscopy during admission revealed severe, diffuse inflammation throughout the colon with visible vessels and adherent clots in the distal colon. She was empirically started on steroids while awaiting infective workup. Given the severity of the disease, biologic therapy was being considered; however, stool PCR was positive for Yersinia enterocolitica, and antibiotics were started. Symptoms initially improved, but a week later, she returned with recurrent bleeding. A repeat colonoscopy revealed worsened inflammation and extremely friable mucosa, preventing completion of the procedure. Due to bleeding and non-healing mucosa, the patient required a subtotal colectomy. Discussion: This case demonstrates the overlap between IBD and infectious colitis. Clinical presentation and endoscopic findings can be misleading, and without confirmatory histopathology or stool studies, misdiagnosis is possible. Initiating corticosteroids in this patient before ruling out infection posed a risk of exacerbating an unrecognized pathogen. Anchoring bias likely played a role in this case. The outpatient history suggested chronicity, and findings on imaging reinforced the pre-existing bias toward IBD. However, the resolution of symptoms following antimicrobial treatment suggests that an infectious etiology was primary. Some studies have shown that up to 15% of patients presenting with presumed IBD flares may have a concurrent infection and were reclassified as non-IBD, once again reiterating to always consider mimics in patients with new or worsening GI symptoms suggestive of IBD.
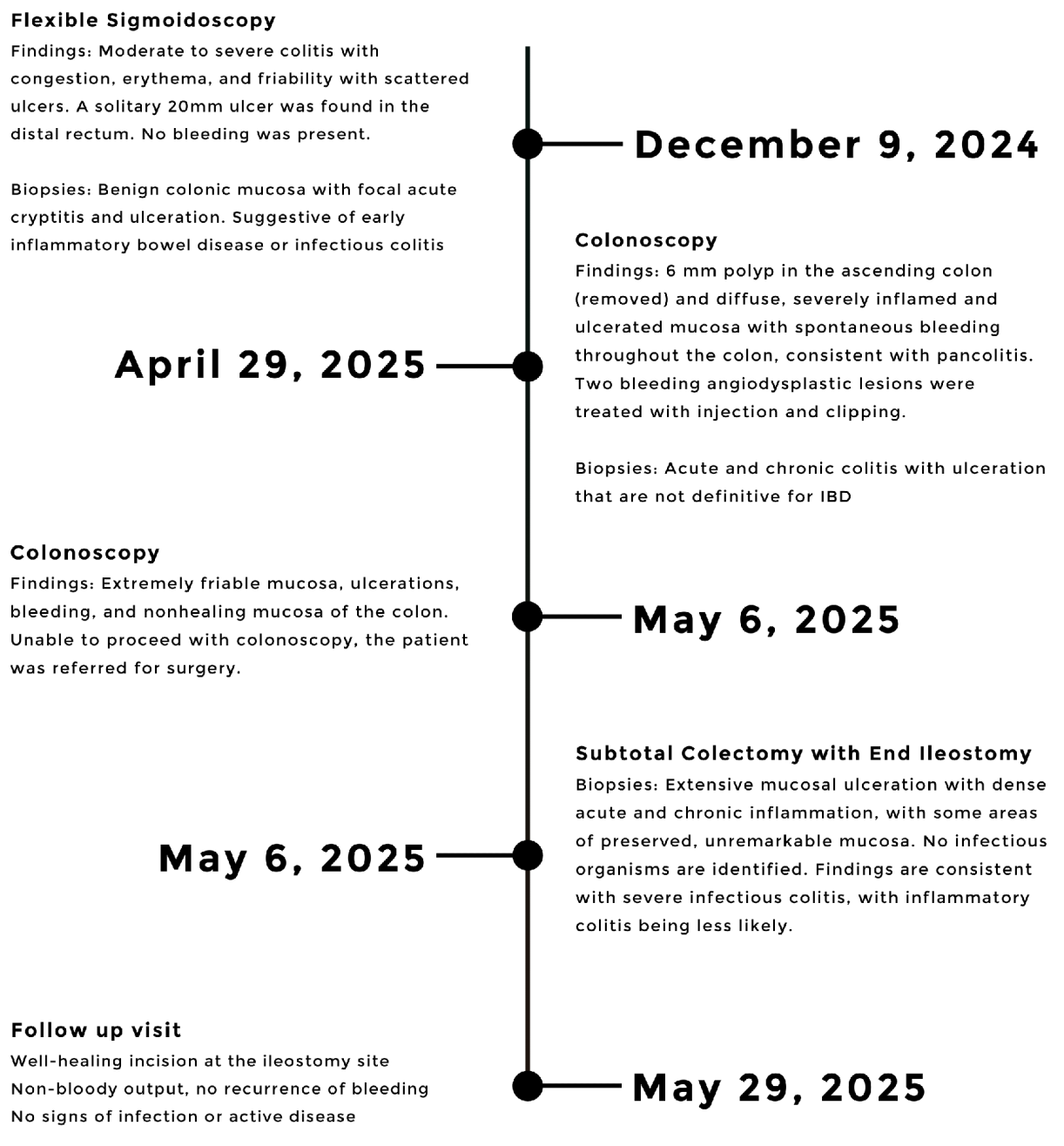
Figure: Figure 1: Chronological timeline of key diagnostic and therapeutic interventions, highlighting procedures and biopsy results.
Disclosures: Maher Taha indicated no relevant financial relationships. Lana Dardari indicated no relevant financial relationships. Arthur Igbo indicated no relevant financial relationships. Amna Naveed Butt indicated no relevant financial relationships. Angelin Raju indicated no relevant financial relationships.
Maher Taha, MD1, Lana Dardari, MD2, Arthur CHIDI. Igbo, MD, MPH3, Amna Naveed Butt, MD4, Angelin Raju, MD5. P5526 - Not All That Bleeds Is IBD: A Case of Yersinia Enterocolitica Mimicking Flare in Suspected Inflammatory Bowel Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.