Texas Tech University Health Sciences Center Tucson, AZ
Letisha M. Bowman, MD1, Meher Gujral, MBBS2, Astin Worden, MD3, Leah A. Swanson, MD4, Talha A. Malik, MD4 1Texas Tech University Health Sciences Center, Amarillo, TX; 2Mayo Clinic, Poughkeepsie, NY; 3Mayo Clinic, Phoenix, AZ; 4Mayo Clinic, Scottsdale, AZ Introduction: Crohn's disease (CD) is a chronic, immune-mediated condition primarily affecting the GI tract but may present with extraintestinal manifestations, including oral Crohn's disease (OCD). OCD can precede, follow or occur concomitantly with GI symptoms, complicating diagnosis and treatment. We present a case of OCD with non-specific lesions in the form of buccal ulcers and maxillofacial pain.
Case Description/
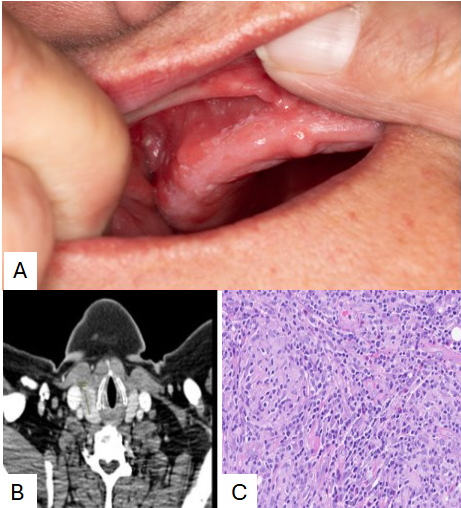
Methods: A 57-year-old female with tobacco use and adult-onset Crohn's ileocolitis on infliximab originally presented with stricturing terminal ileal disease complicated by recurrent small bowel obstructions. She was treated with dose escalation of infliximab to 5mg/kg every 6 weeks, which led to clinical remission. Ten years later, she presented with right-sided facial pain, buccal ulcers, and intraoral lesions of the lip, gums, and tongue (Image A). A biopsy showed granulomatous inflammation. She self-discontinued infliximab as she thought it was the culprit. She did not respond to dexamethasone oral solution and gabapentin. Metronidazole, minocycline and intralesional triamcinolone yielded partial response but oral pain, poor oral intake, and weight loss persisted.
She was admitted for worsening oral pain and new obstructive symptoms. Abdominal CT revealed small bowel obstruction. Maxillofacial CT showed extensive inflammatory changes involving the right buccal mucosa (Image B). Repeat mucosal biopsy showed granulomatous inflammation (image C) with negative AFB and fungal stains. She was treated with IV steroids and restarted on infliximab 10 mg/kg monthly. She quit smoking and nutrition was optimized. Her oral lesions resolved over weeks, but persistent fibrostenotic strictures necessitated ileocecectomy. She maintained clinical remission postoperatively on infliximab every 6 weeks and azathioprine.
Discussion: OCD is seen in up to 37% of adult CD patients and often presents with non-specific lesions. Differentiation from Behçet's, sarcoidosis and infection is crucial. Nutritional deficiencies, present in 65-70% of CD patients, can be exacerbated by oral symptoms. Nutritional optimization, including treatment of micronutrient deficiencies,is paramount. Smoking impacts CD and cessation reduces relapse and surgery risk, warranting counseling and nicotine replacement therapy. This case highlights the need for a multi-disciplinary approach including aggressive disease control, nutritional optimization and smoking cessation to achieve intestinal disease control and improving long-term outcomes.
Figure: A) Ulcerated buccal mucosa ulcer B) Maxillofacial CT scan showing a 15.1mm right granulomatous lesion C) Granulomatous inflammation of mucosal biopsy suggestive of Crohn’s Disease.
Disclosures: Letisha Bowman indicated no relevant financial relationships. Meher Gujral indicated no relevant financial relationships. Astin Worden indicated no relevant financial relationships. Leah Swanson indicated no relevant financial relationships. Talha Malik indicated no relevant financial relationships.
Letisha M. Bowman, MD1, Meher Gujral, MBBS2, Astin Worden, MD3, Leah A. Swanson, MD4, Talha A. Malik, MD4. P5509 - Beyond the Bowels: A Case of Oral Crohn’s Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")