University of British Columbia Department of Medicine Surrey, BC, Canada
Bachviet AH. Nguyen, MD1, Astrid-Jane Williams, MD2, Gregory Rosenfeld, MD, MHSc2 1University of British Columbia Department of Medicine, Surrey, BC, Canada; 2UBC Department of Medicine/IBD Centre of BC, Vancouver, BC, Canada Introduction: Danon disease is an X-linked dominant mutation of the LAMP2 gene manifesting with progressive hypertrophic cardiomyopathy, progressive proximal muscle weakness, and cognitive impairment.
Herein, we describe the first reported association of Crohn's disease (CD) and Danon disease.
Case Description/
Methods: A 19 year old male with a history of infiltrative hypertrophic cardiomyopathy secondary to Danon disease presented with an exacerbation of intermittent chronic diarrhea of 2 years’ duration. The patient had increasing loose stools 1 month after an elective orthoptic cardiac transplant for Danon disease. His symptoms were stress-induced with occasional hematochezia but there was no tenesmus or urgency. He reported pain in the upper gluteal fold close to the coccyx when straining. Current medications included mycophenolate mofetil and tacrolimus. His physical exam was normal while a stool culture, ova & parasites, cytomegalovirus (CMV) PCR and a tacrolimus level were unremarkable.
To exclude post-transplant CMV colitis, a colonoscopy was performed which demonstrated a normal ileum but cobblestoning of the mucosa throughout the colon suggestive of CD. Biopsies of the transverse and descending colon confirmed severe chronic active colitis with ulceration and immunohistochemical staining negative for CMV infection. The patient was started on oral prednisone and sulfasalazine with subsequent symptomatic relief.
Unfortunately, the patient later developed recurrent CD flares. Several pelvic MRIs following the initial colonoscopy demonstrated chronic perianal fistula over the next two years with treatment failure on sulfasalazine, vedolizumab, adalimumab, and infliximab. Ustekinumab was effective in inducing remission of his CD. The fistula was managed with seton placement and antibiotics. Discussion: We described a new diagnosis of colonic and perianal fistulising CD in a patient with Danon disease. Interestingly, the patient demonstrated active colonic disease post-cardiac transplant while on immunosuppressive mycophenolate mofetil and tacrolimus.
Infectious causes should be excluded in a patient with Danon disease presenting with diarrhea, but the possibility of inflammatory bowel disease should also be considered.
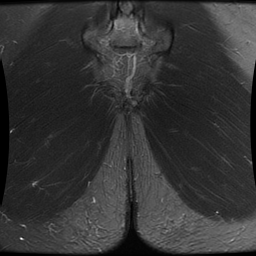
Figure: Figure 1: Coronal section of a T2 MRI perianal fistula protocol demonstrating a high-signal T2 intense tract that extends caudally in the intersphincteric space, suggesting a perianal fistula. The complete scan suggested a high intersphincteric fistula (Saint James grade 2) with a secondary tract more caudally.
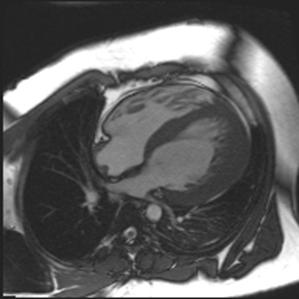
Figure: Cardiac MRI without contrast taken 3 years prior to the initial cardiac transplant demonstrating hypertrophic cardiomyopathy with preserved systolic function. The left ventricular myocardial mass index was 262.5 grams/meter sq. The left ventricular end-diastolic volume index was 86.2 cc. The end systolic volume index was 28.8 cc. The stroke volume index was 57.4 cc. Ejection fraction was 66.6% and the cardiac index was 3.8 L per min per m squared.
Disclosures: Bachviet Nguyen indicated no relevant financial relationships. Astrid-Jane Williams indicated no relevant financial relationships. Gregory Rosenfeld indicated no relevant financial relationships.
Bachviet AH. Nguyen, MD1, Astrid-Jane Williams, MD2, Gregory Rosenfeld, MD, MHSc2. P5508 - A Novel Association of Danon Disease and Crohn’s Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Bachviet AH Nguyen, MD (he/him/his) photo")