Mina Awadallah, MD, MSc1, John Fang, MD1, John Erikson Yap, MD, MBA, FACG2 1University of Utah, Salt Lake City, UT; 2University of Utah Health, Salt Lake City, UT Introduction: Post-procedure bleeding at a PEG site can usually be managed with local external and internal endoscopic methods. When the bleeding site cannot be localized externally or intraluminally by endoscopy conventional hemostatic strategies may be less effective. In addition, impaired wound healing due to underlying connective tissue disease, such as hypermobile Ehlers-Danlos Syndrome (hEDS), and malnutrition may also limit the effectiveness of these methods . We describe a novel dual site approach to post-PEG bleeding using RADA16, a self-assembling peptide hydrogel, applied both endoscopically and externally to control bleeding while maintaining PEG function.
Case Description/
Methods: A 21-year-old woman with hEDS, malnutrition and Mast Cell Activation Syndrome (MCAS) presented with persistent oozing bleeding and pain at her PEG site one week following a PEG tube exchange. Her history included multiple episodes of buried bumper syndrome, and she remained dependent on both PEG (for venting) and DPEJ (direct percutaneous endoscopic jejunostomy) tube and TPN for nutrition support. A week-long conservative effort including bolster adjustments, dry dressings, and pressure dressings were unsuccessful. Due to the necessity of PEG access and the localized nature of the bleeding, endoscopic evaluation was pursued.
Upper endoscopy showed active oozing at the internal PEG site without exact site of bleeding identified. The PEG was removed under direct visualization. A topical hemostatic matrix was applied both intraluminally at the fistula and externally at the stoma. Complete hemostasis was achieved. The same 16 Fr gastrostomy tube was reinserted through the mature tract. Position was confirmed endoscopically. The site was cleaned and dressed. No immediate or delayed complications including re-bleeding occurred. Discussion: This case highlights an effective and innovative approach to managing bleeding at a PEG site in a medically complex patient. Traditional hemostatic interventions may be insufficient when bleeding occurs between the external stoma opening and internal PEG fistula. The successful use of a topically applied hemostatic matrix applied both internally and externally controlled bleeding without requiring extended tube removal or tract closure thus preserving PEG access. This dual-application strategy offers a minimally invasive solution and may have broader applications in similar high-risk clinical scenarios where conventional options are limited.
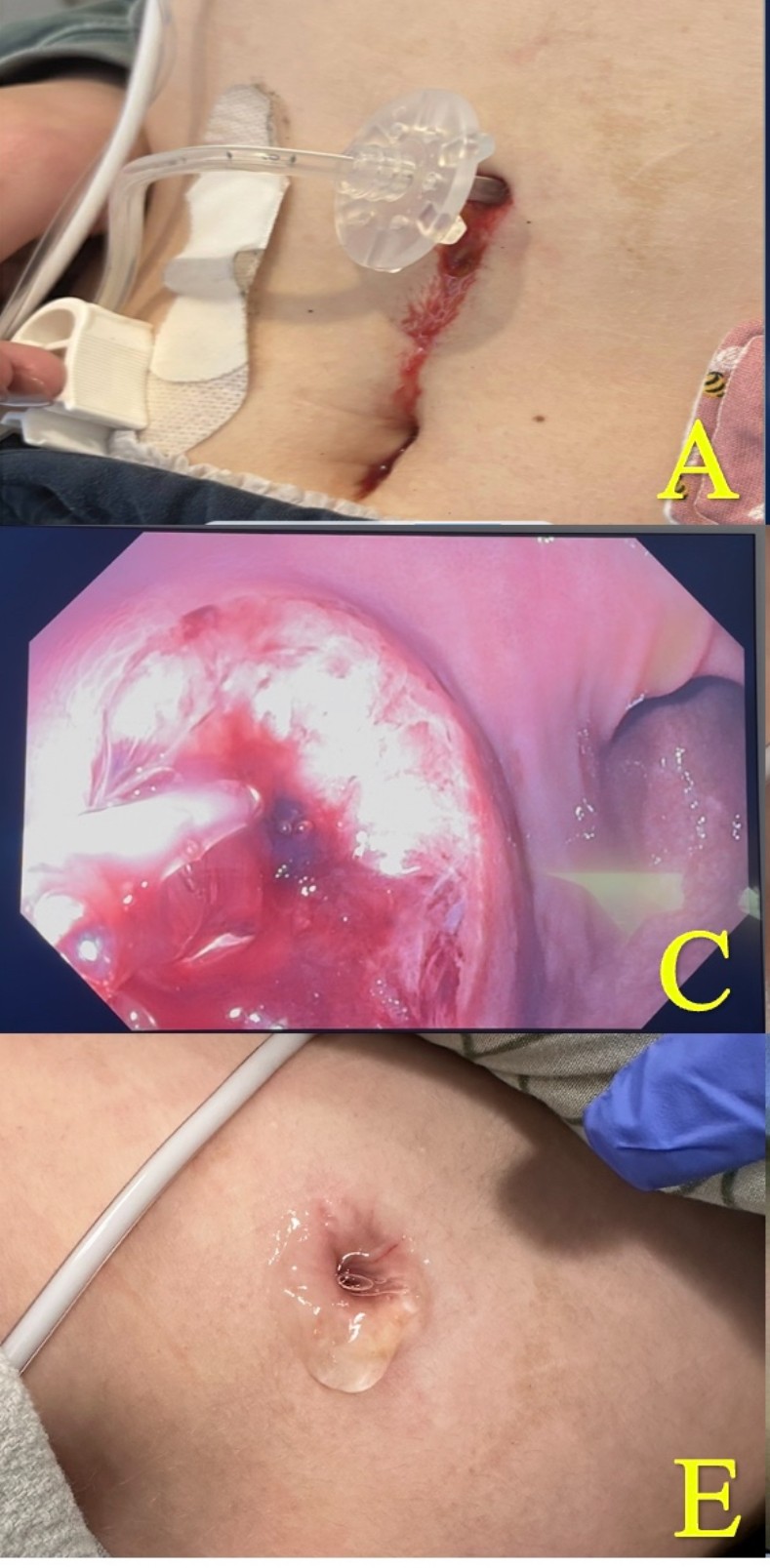
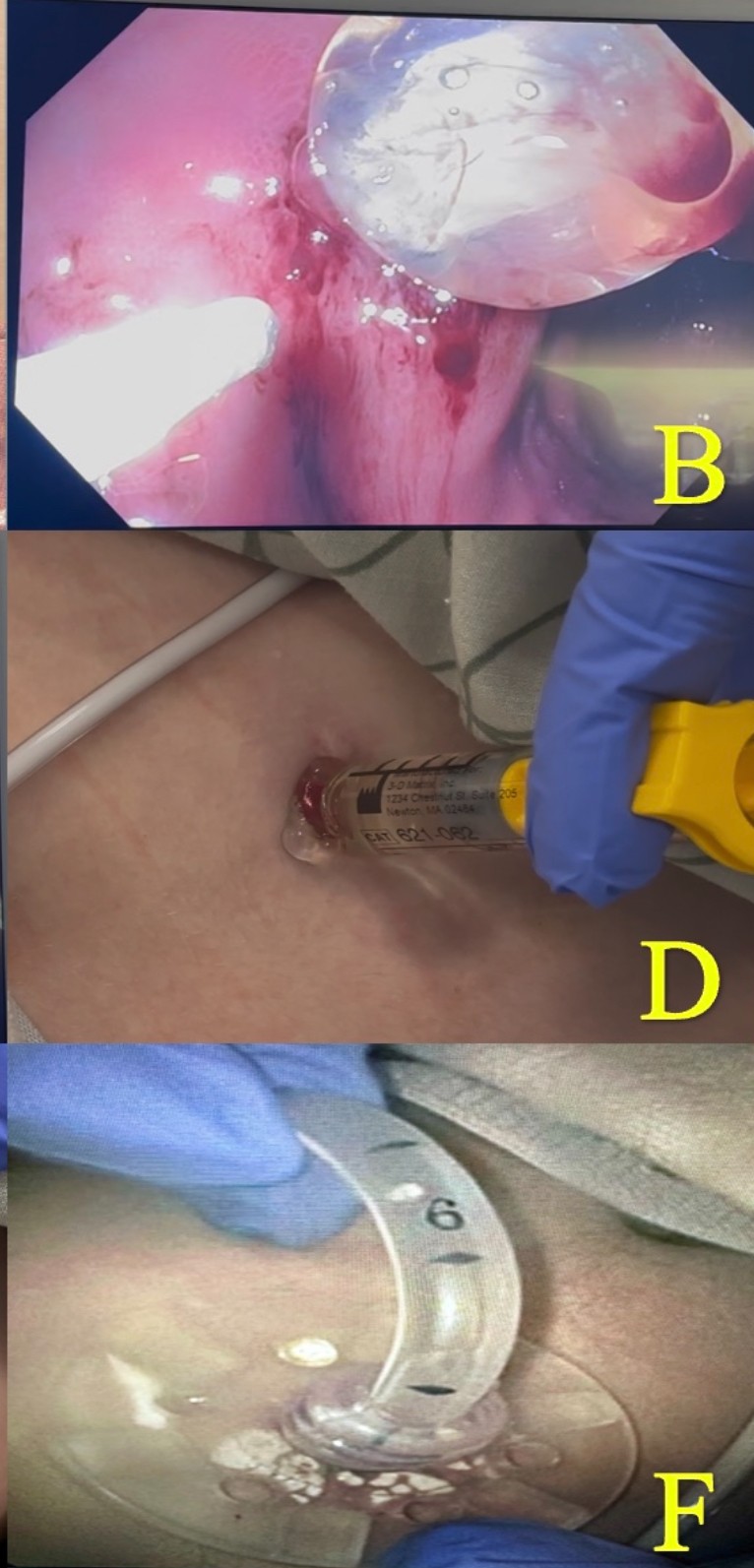
Figure: A.Cutaneous view of oozing G tube site. C.Endoscopic application of RADA16. E.Complete hemostasis achieved.
Figure: B.Endoscopic view of oozing G tube site. D.Cutaneous application of RADA16. F.Replacement of G tube.
Disclosures: Mina Awadallah indicated no relevant financial relationships. John Fang: Aspero Medical – Consultant. Circa Scientific – Consultant. Merit – Consultant. John Erikson Yap: Phathom Pharmaceutical – Speakers Bureau. Steris – Consultant.
Mina Awadallah, MD, MSc1, John Fang, MD1, John Erikson Yap, MD, MBA, FACG2. P5293 - Innovative Management of Percutaneous Endoscopic Gastrostomy (PEG) Bleeding in a Patient With Malnutrition and Impaired Healing Using RADA16, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.