Marshall University Joan C. Edwards School of Medicine Huntington, WV
Elizabeth Harris, MD1, Mohamed Alshal, MD2, Ali Saad Elharari Mohamed, MD3, Rahoma Saad, MD2 1Marshall University Joan C. Edwards School of Medicine, Huntington, WV; 2Marshall University - - Huntington, WV, Huntington, WV; 3University of Tripoli, Tripoli, Tripoli, Libya Introduction: A rectal mass causing rectal bleeding is most commonly rectal adenocarcinoma, though other malignancies and benign lesions are also in the differential diagnosis. Extramedullary hematopoiesis is rarely found in the gastrointestinal (GI) luminal tract and has not previously been reported as a cause of lower GI bleeding. We report a case of a rectal bleeding from a rectal mass due to extramedullary hematopoiesis in the setting of chronic myelomonocytic leukemia 1 (CMML-1).
Case Description/
Methods: A 67-year-old male with CMML-1 managed with supportive care and high-risk stage IIC prostate cancer status post external beam radiation therapy, presented to the Emergency Department with rectal bleeding. His initial lab results showed a hemoglobin of 11.4 gm/dL, white blood cell count of 47.7 k/cm2, and platelet count of 48 k/cm2. Computed tomography abdomen pelvis revealed splenomegaly and thickening of the inferior rectum with presacral fat stranding. Of note, six months prior, he presented with rectal bleeding and underwent colonoscopy that showed localized angiodysplastic lesions with bleeding on contact in the mid-rectum, consistent with radiation proctitis, that were successfully treated with coagulation for tissue destruction using argon plasma.
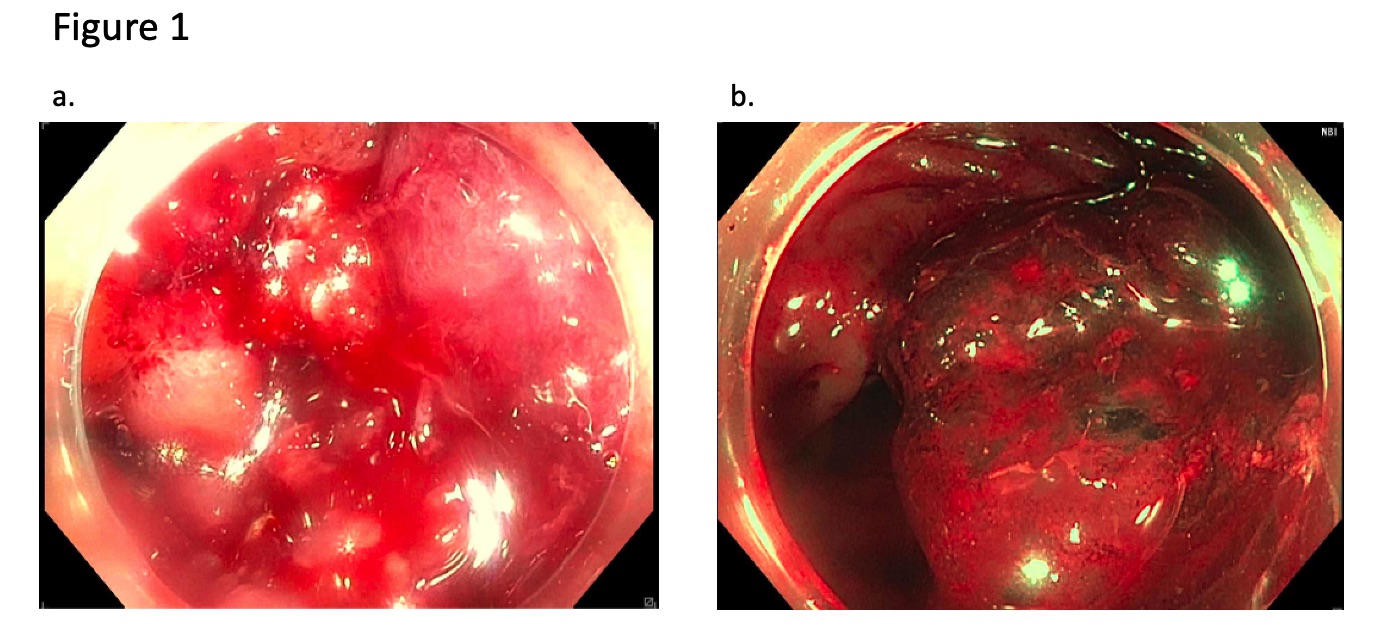
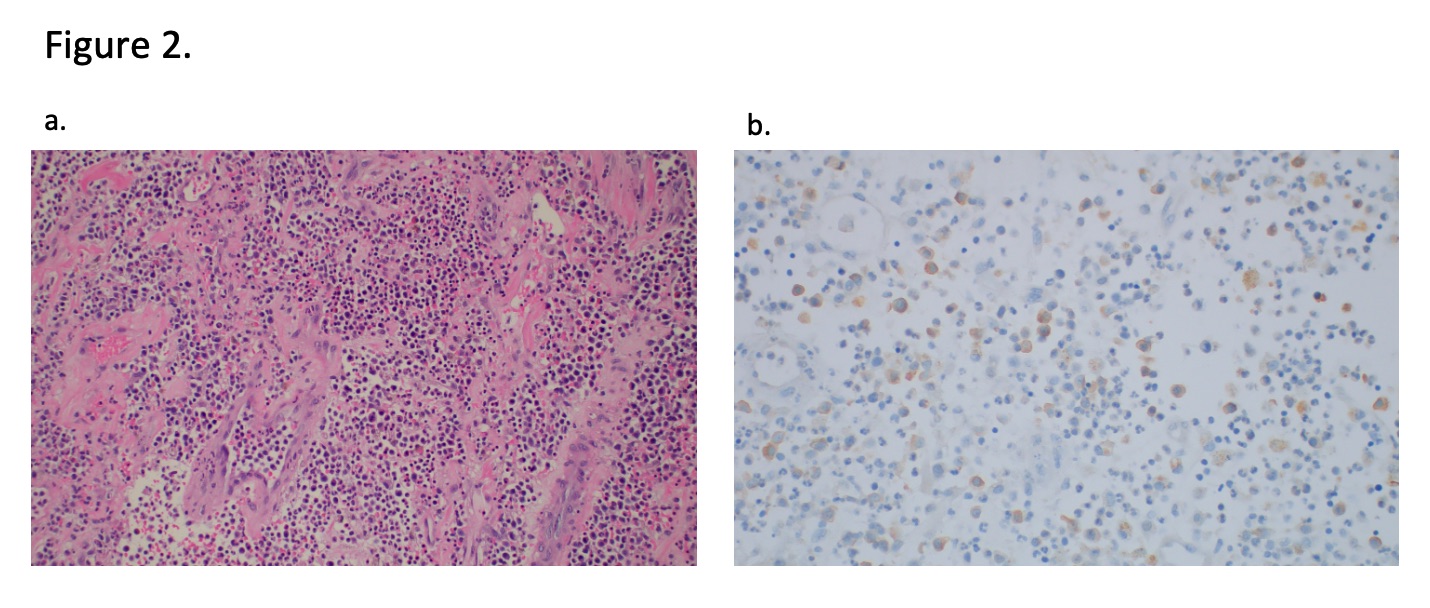
On this presentation, he was admitted and underwent repeat colonoscopy that showed a villous, fungating, polypoid mass in the rectum (Figure 1a-b). The mass was oozing and partially circumferential, measuring twenty millimeters in length and twenty-five millimeters in diameter. Biopsy demonstrated a diffuse mixed cellular infiltrate composed of maturing granulocytic cells, erythroid precursors, and megakaryocytes. The infiltrate showed granulocytic predominance with left shift and scattered aggregates of immature mononuclear cells. (Figure 2a-b) Necrotic rectal mucosa, fibrosis, and hemorrhage were present in the background, consistent with infarct changes. Stains were consistent with abnormal extramedullary hematopoiesis in the setting of CMML. A repeat bone marrow biopsy confirmed persistent CMML-1 with 3% blasts. The patient was treated with five cycles of decitabine for CMML-1 resulting in complete resolution of rectal bleeding. Discussion: Rectal mass biopsy in this patient showed a previously undescribed cause of rectal mass – extramedullary hematopoiesis. This case highlights an unusual cause for lower GI bleeding, but one that is important to consider in patients with myeloproliferative or myelodysplastic disorders.
Figure: Figure 1. a. Endoscopic image of villous, fungating, and oozing rectal mass b. Endoscopic image of mass under narrow band imaging
Figure: Figure 2. a. Hematoxylin and eosin (H&E) stain (200X original magnification) shows cellular proliferation is composed of a mixture of myeloid cells with left shift, fewer erythroid precursors, and rare megakaryocytes. b. Myeloperoxidase stain highlights myeloid cells.
Disclosures: Elizabeth Harris indicated no relevant financial relationships. Mohamed Alshal indicated no relevant financial relationships. Ali Saad Elharari Mohamed indicated no relevant financial relationships. Rahoma Saad indicated no relevant financial relationships.
Elizabeth Harris, MD1, Mohamed Alshal, MD2, Ali Saad Elharari Mohamed, MD3, Rahoma Saad, MD2. P5279 - An Unusual Cause of Rectal Bleeding: Rectal Mass from Abnormal Extramedullary Hematopoiesis in the Setting of Chronic Myelomonocytic Leukemia, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.