Staten Island University Hospital, Northwell Health Staten Island, NY
Daniel Kallta, DO, Ryan Njeim, MD, Youssef El Douaihy, MD Staten Island University Hospital, Northwell Health, Staten Island, NY Introduction: Hemosuccus pancreaticus (HP) is a rare, life-threatening cause of upper gastrointestinal bleed (UGIB) caused by hemorrhage into the pancreatic duct with blood oozing from the ampulla of Vater. We report a case of HP due to a pancreatic pseudocyst in a patient with complex comorbidities.
Case Description/
Methods: A 60-year-old woman with a history of alcohol-induced pancreatitis, pancreatic duct (PD) dilation, and a known benign pancreatic head cyst presented with acute shortness of breath and back pain. Imaging revealed bilateral pulmonary emboli with right heart strain and she underwent catheter-directed thrombectomy. Due to persistent hypotension and back pain, a computed tomography (CT) scan of the abdomen and pelvis was performed showing persistent pancreatic ductal dilation, stable pancreatic head cyst and a new 8.8 cm cystic lesion near the pancreatic tail concerning for pseudocyst or neoplasm. Lipase was 779 U/L so the patient was diagnosed with acute pancreatitis and treated with intravenous fluids.
Two days later, she developed hematemesis and hematochezia with hemoglobin drop (11.6 8.6 g/dL). An esophagogastroduodenoscopy (EGD) showed normal esophageal and gastric mucosa; however, careful inspection revealed active oozing of fresh blood from the major duodenal papilla, highly suggestive of HP. Interventional radiology (IR) and surgery were urgently consulted and a CT angiography revealed a growing pancreatic head lesion without active extravasation. Anticoagulation was held and an IVC filter was placed. The bleeding subsequently resolved with supportive measures alone and no intervention was needed. The patient still complained of persistent abdominal pain and inability to tolerate oral intake, thus, an EUS was performed showing a large pancreatic pseudocyst. An EUS-guided cystogastrostomy was performed with successful lumen-apposing metal stent (LAMS) placement, with improvement of patient’s symptoms. The patient was discharged with close follow-up. Three weeks later, follow-up EGD confirmed resolution of the pseudocyst and the LAMS was removed without complication nor recurrence of bleed. Discussion: We describe a rare cause of UGIB caused by HP likely due to pseudocyst-related vessel erosion without pseudoaneurysm. HP is usually treated with embolization or surgical intervention; however, it can be self-limited. HP should be considered for patients with obscure UGIB, especially in those with underlying pancreatic disease and suggestive imaging findings.
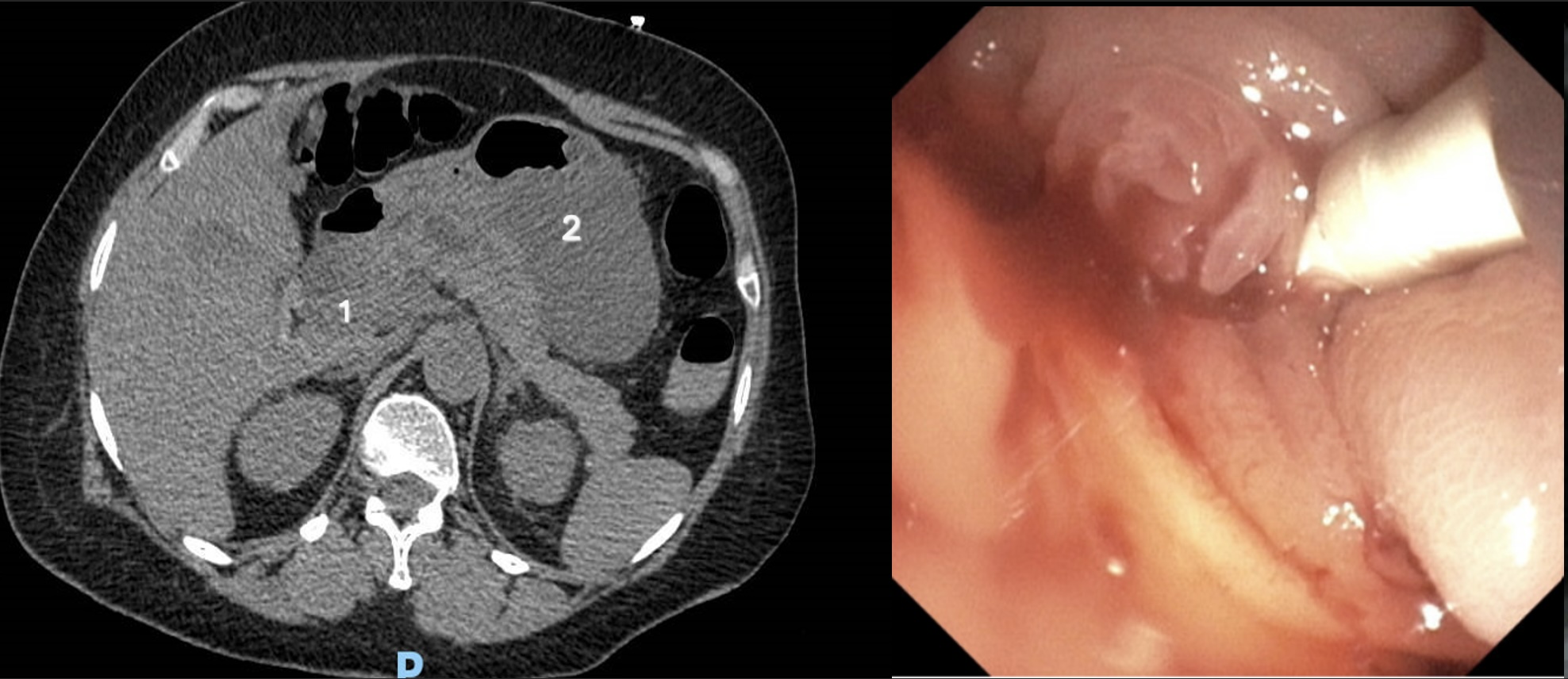
Figure: On the left, CTA showing pancreatic cyst (1) and pseudocyst (2). On the left bleeding from papilla on EGD
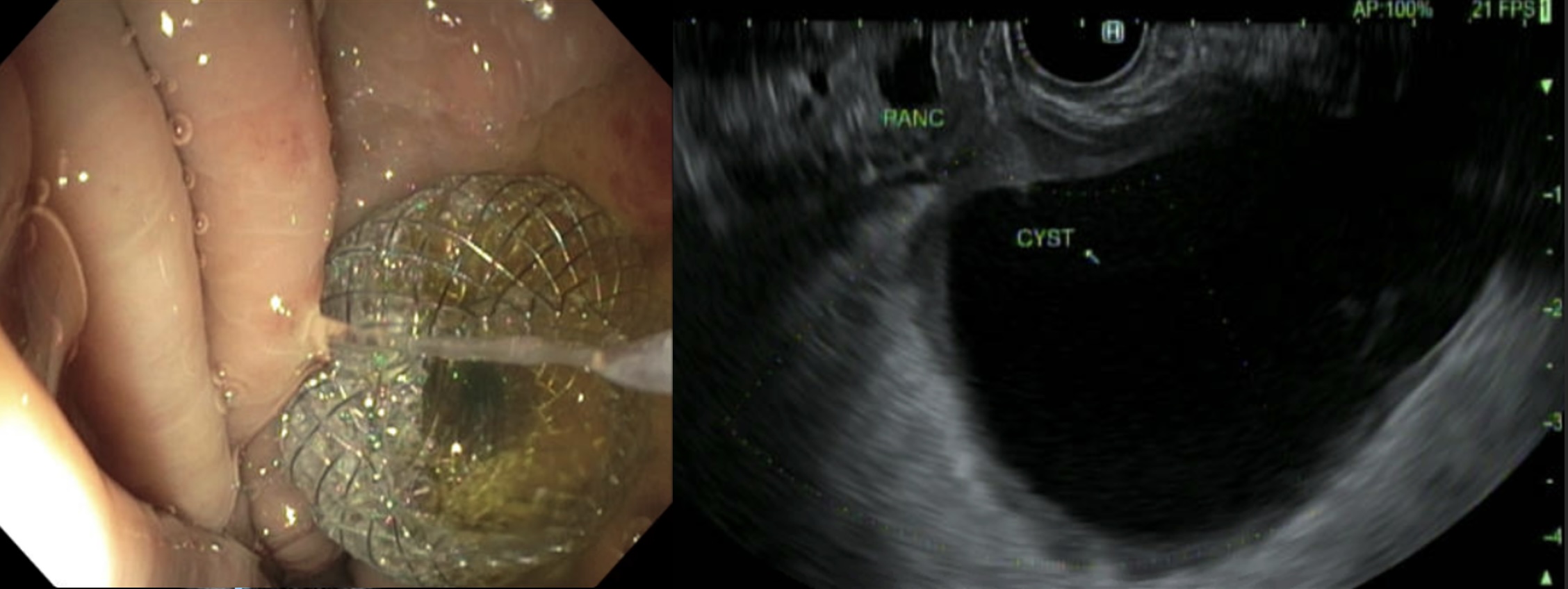
Figure: On the left, Axios in place, on the right, EUS image of pseudocyst
Disclosures: Daniel Kallta indicated no relevant financial relationships. Ryan Njeim indicated no relevant financial relationships. Youssef El Douaihy indicated no relevant financial relationships.
Daniel Kallta, DO, Ryan Njeim, MD, Youssef El Douaihy, MD. P5250 - Hemosuccus Pancreaticus: A Rare Cause of Gastrointestinal Bleeding, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.