University of Kentucky College of Medicine Lexington, KY
Ren Bryant, DO1, Alyssa Lambrecht, DO2, Lucas Roy, MD1 1University of Kentucky College of Medicine, Lexington, KY; 2University of Kentucky, Lexington, KY Introduction: Acute GI bleeding is a common presentation for patient admission. Patients usually have risk factors such as recent antiplatelet therapy, anticoagulation, helicobacter pylori infection, non-steroidal anti-inflammatory (NSAID), corticosteroid, or alcohol use. While gastric ulcerations have a broad differential, amyloid ulcerations are exceedingly rare with an incidence of 1%. Amyloidosis is caused by abnormal extracellular tissue deposition of fibers in various organs. Here we present a case of a patient with an acute upper GI bleeding from progression of AL amyloidosis into gastric tissue.
Case Description/
Methods: A 62-year-old male with recent diagnosis of AL-amyloidosis (ALA) complicated by nephrotic syndrome, left ventricular hypertrophy, and recurrent pleural effusions presented with 3 days of dyspepsia, nausea, “coffee-ground” emesis, and melanic stools. He denied any recent NSAID, alcohol, anticoagulation or steroid use. While vitals were stable, his hemoglobin had trended down to 11.5 from 13.1 two weeks prior. Initial International Normalized Ratio (INR) and prothrombin time were normal and h. pylori stool antigen was negative. An esophagogastroduodenoscopy (EGD) was performed and found a large, circumferential antral ulceration with diffusely oozing hemorrhage (Forrest IB) temporized with epinephrine and hemostatic powder with achieved hemostasis. He was treated with a Proton Pump Inhibitor (PPI) drip for 72 hours and transitioned to an oral PPI regimen. Biopsies of the ulcer were positive for ALA. The patient had clinical improvement and resolution of symptoms prior to discharge. Discussion: Classified as a rare disease, ALA is known to have a wide range of possible etiologies and clinical manifestations, most commonly the heart and kidney. In 2018, incidence of ALA is between 9.7 to 14.0 cases per million person/year in the United States. The gold standard remains tissues biopsy with apple green birefringence on a Congo red stain. While there are no specific guidelines on PPI duration in gastric ALA, it is reasonable to follow current PPI guidelines. Since chemotherapy treatments for amyloid cannot reverse tissue damage the duration of PPI treatment may need to be individualized per patient. More research needs to be done to monitor the risk of rebleeding and optimal duration of PPI use in patients with ALA induced gastric ulcers. Though rare, this case argues for inclusion of ALA related gastric ulcers in the clinician’s diagnostic differential.
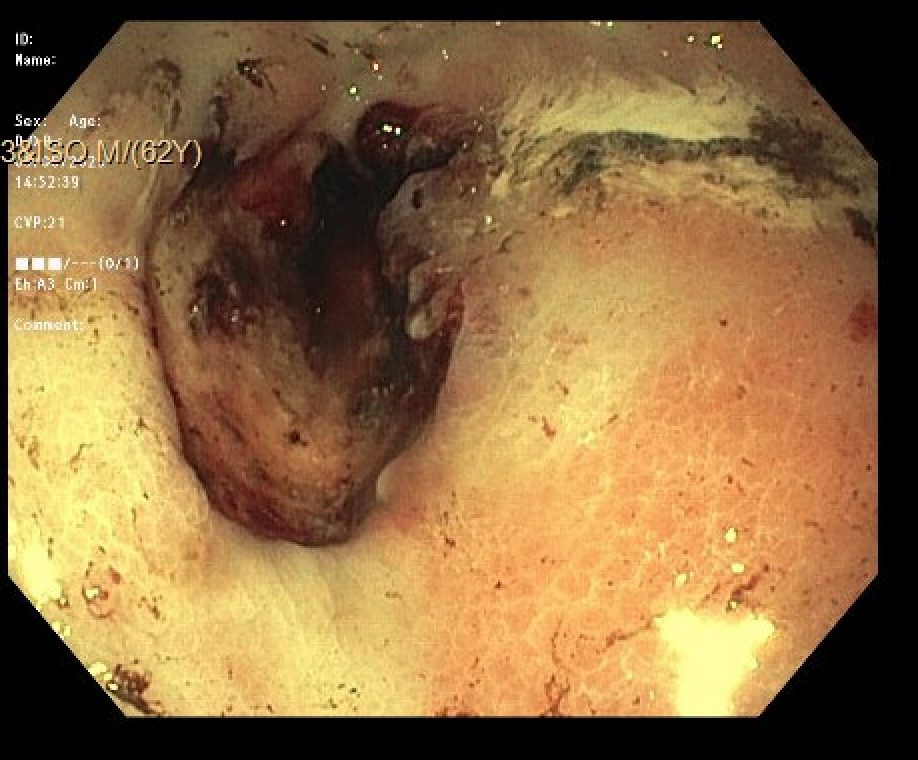
Figure: Gastric ulcer without bleeding
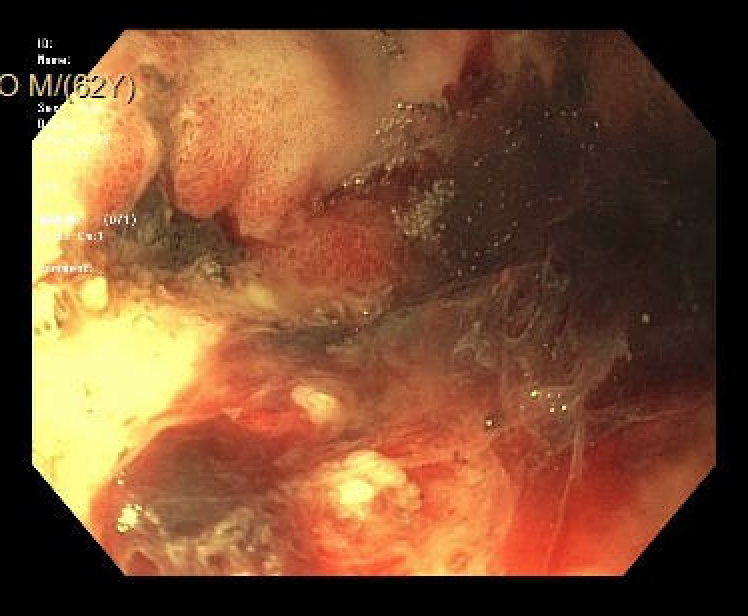
Figure: Gastric ulcer with active oozing
Disclosures: Ren Bryant indicated no relevant financial relationships. Alyssa Lambrecht indicated no relevant financial relationships. Lucas Roy indicated no relevant financial relationships.
Ren Bryant, DO1, Alyssa Lambrecht, DO2, Lucas Roy, MD1. P5246 - A Case of Gastric Ulcer Amyloid Light Chains (AL) Amyloidosis: A Cause of Acute Gastrointestinal (GI) Bleeding, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")