University of Missouri - Kansas City School of Medicine Kansas City
Zaid Al Momani, MD, Aron Evans, MD, Laith Al Momani, MD University of Missouri - Kansas City School of Medicine, Kansas City, MO Introduction: Gastric outlet obstruction (GOO) is characterized by mechanical blockage preventing gastric contents from passing into the small intestine, and one underrecognized cause of GOO is gastrostomy tube (GT) malposition. We present a case of GOO resulting from GT balloon migration beyond the pylorus that was identified by direct visualization after multiple negative computed tomography (CT) scans and was corrected endoscopically.
Case Description/
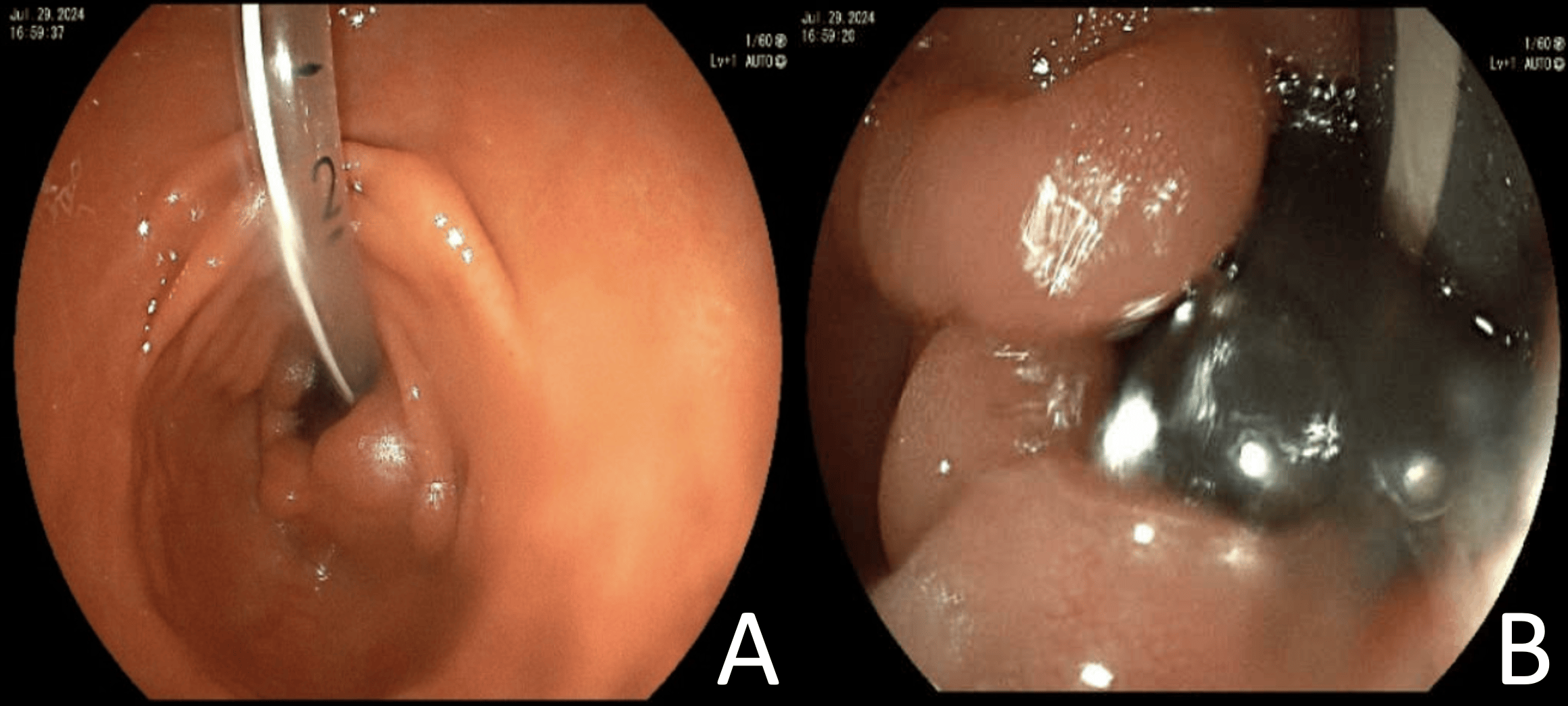
Methods: A 66-year-old nonverbal female admitted for a urinary tract infection developed recurrent vomiting and abdominal pain with tube feedings. She was 11 months status-post laparoscopic-assisted GT placement following a diagnosis of autoimmune encephalitis and poor oral intake. Ever since placement, she developed recurrent nausea, vomiting, and abdominal pain, leading to multiple emergency room visits and a total of 11 CT scans (several utilizing enteric contrast dye) which all showed appropriate positioning of the GT within the stomach. Inpatient gastroenterology service was consulted and repeat CT of the abdomen and pelvis with intravenous contrast was consistent with prior imaging. Direct visualization with esophagogastroduodenoscopy revealed that the internal balloon was lodged at the pylorus/proximal bulb (Figure 1). This highlighted the possibility of intermittent migration of the GT, causing GOO and delivering bolus feeds directly into the duodenum. The balloon was subsequently deflated with a syringe, repositioned against the stomach wall, and re-inflated under endoscopic guidance. The patient’s symptoms completely resolved with no reported tube feed intolerance or need for abdominal imaging for nearly 1 year. Discussion: GTs are commonly placed in patients who require long-term enteral nutrition. While malposition is rare, it can lead to GOO. This case demonstrates an unusual presentation of intermittent GOO with frequent isolated episodes over several months and multiple imaging studies showing an appropriately positioned GT. This highlights the challenges in detection, and the importance of having a high level of suspicion for the intermittent nature of obstruction while combining bedside, imaging, and endoscopic evaluations to diagnose this complication. Management is often safe and simple with repositioning of the tube and its' external bumper.
Figure: Figure 1: Image A and B showing the percutaneous endoscopic gastrostomy tube internal balloon lodged in the duodenum.
Disclosures: Zaid Al Momani indicated no relevant financial relationships. Aron Evans indicated no relevant financial relationships. Laith Al Momani indicated no relevant financial relationships.
Zaid Al Momani, MD, Aron Evans, MD, Laith Al Momani, MD. P5169 - Unusual Case of Intermittent Gastric Outlet Obstruction Due to Gastrostomy Tube Migration, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.