University of Colorado Anschutz Medical Campus Aurora, CO
Malique Delbrune, MD1, Thomas Enke, MD2, Blake Niccum, MD1, Mohammad Bilal, MD, FACG3 1University of Colorado Anschutz Medical Campus, Aurora, CO; 2University of Colorado, Aurora, CO; 3University of Colorado Anschutz Medical Campus, Denver, CO Introduction: ngestion of a foreign body is common and frequently requires medical evaluation. Treatment is determined by the patient’s symptoms, timing of ingestion, and item’s size, material, location, and risk of perforation. We present a case of an unintentional ingestion of dentures resulting in hypopharyngeal perforation.
Case Description/
Methods: A 50-year-old female presented after accidental ingestion of her denture. She developed progressive dysphagia, odynophagia, and shortness of breath prompting presentation to an outside hospital. Computed tomography (CT) of the neck with intravenous (IV) contrast revealed thickening of the upper esophagus with retained fluid and debris, however no radiopaque foreign body or perforation were identified. Upper endoscopy (EGD) revealed a denture embedded into the hypopharyngeal wall approximately 15 cm from the incisors. Attempts at removal were deferred, she was started on IV antibiotics and transferred to our tertiary care center for consideration of endoscopic removal.
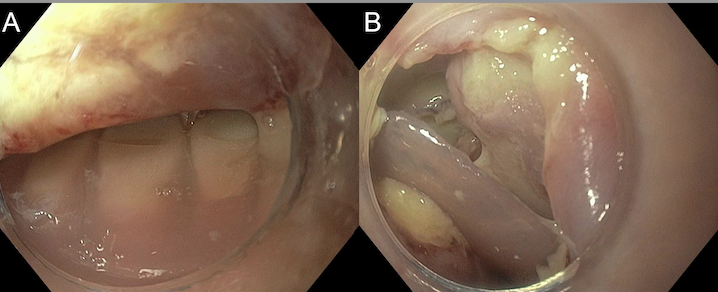
EGD following transfer redemonstrated an embedded denture approximately 15 cm from the incisors, immediately proximal to the upper esophageal sphincter. The associated mucosa was ulcerated and lined with purulent material without clear full thickness perforation (Figure 1). Following discussion with thoracic surgery and otolaryngology the decision was made to proceed with endoscopic removal. The denture was removed with a specialized foreign body hood and grasping forceps. A full thickness perforation was not clearly visualized. Nasogastric (NG) tube was placed under endoscopic guidance. She remained intubated, kept strict nil per os (NPO), and continued IV antibiotics.
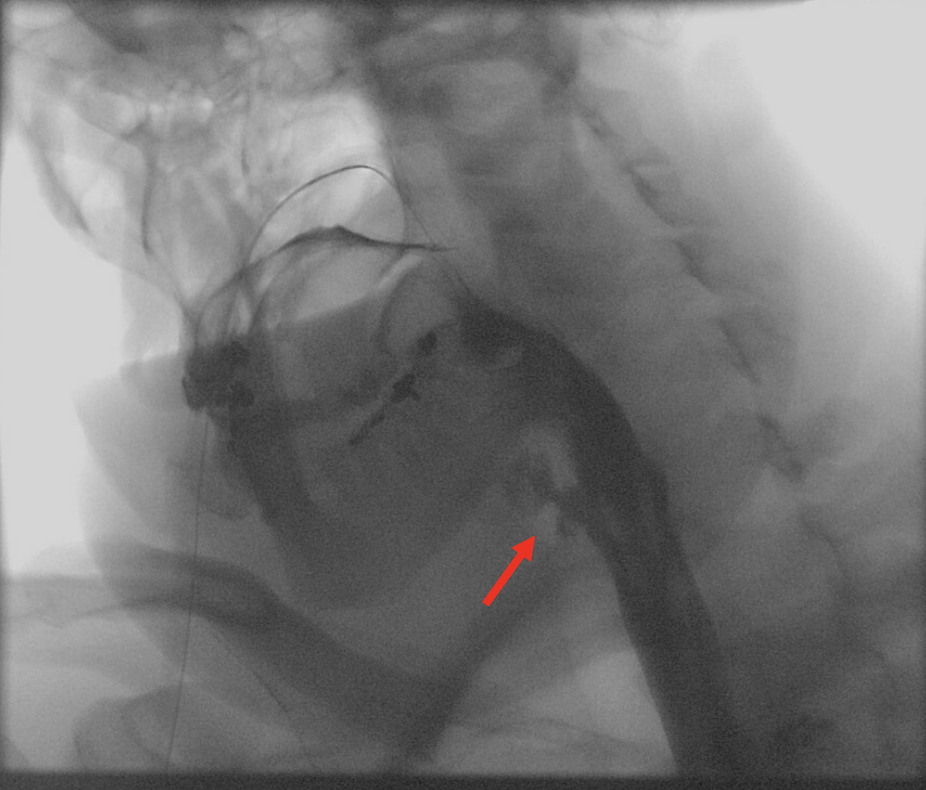
She was extubated post-operative day (POD) 2. CT scan of the neck with IV contrast showed extraluminal gas concerning for a perforation. Conservative management was continued given clinical stability. Repeat EGD performed POD 5 for NG replacement revealed ulcerated mucosa with overlying granulation tissue. Esophagram on POD 6 revealed persistent leak (Figure 2). Conservative management was continued. No leak was identified on POD 11. Her diet was advanced, and she was discharged POD 13. Discussion: Retained foreign bodies in the hypopharynx can be retrieved endoscopically, though management should include input from thoracic surgery and otolaryngology. We highlight that select cases of hypopharyngeal perforations can be managed non-operatively with antibiotics and strict NPO status.
Figure: Figure 1. Partial denture embedded in the hypopharynx (A) and subsequent removal (B).
Figure: Figure 2. Esophagram demonstrating persistent leak (red arrow) from a hypopharyngeal perforation.
Disclosures: Malique Delbrune indicated no relevant financial relationships. Thomas Enke indicated no relevant financial relationships. Blake Niccum indicated no relevant financial relationships. Mohammad Bilal: Boston Scientific – Consultant. Cook endoscopy – Paid speaker. Steris Endoscopy – Consultant.
Malique Delbrune, MD1, Thomas Enke, MD2, Blake Niccum, MD1, Mohammad Bilal, MD, FACG3. P5154 - False Teeth Perforating a True Lumen: A Story of a Denture Adventure With Hypopharyngeal Perforation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")