Brown University / Rhode Island Hospital Providence, RI
Andrew L. Petrou, MD1, Alex Chang, MD1, Priya Kumari Maheshwari, MD2, Li Wang, MD1 1Brown University / Rhode Island Hospital, Providence, RI; 2University of Central Florida, HCA Healthcare GME, Pensacola, FL Introduction: Merkel cell carcinoma (MCC) is a rare, aggressive neuroendocrine malignancy of the skin, primarily affecting elderly and immunosuppressed individuals. Characterized by a high rate of local recurrence and distant metastasis, MCC most commonly spreads to lymph nodes, liver, lungs, and bone. However, presentations with nonspecific symptoms such as abdominal pain and esophagogastric junction outflow obstruction (EGJOO) are exceedingly uncommon and can obscure timely diagnosis. This case report describes a unique presentation of MCC in a patient who presented with epigastric pain and was subsequently found to have metastatic involvement of the celiac axis lymph nodes, highlighting the diagnostic challenges and importance of considering MCC in the differential diagnosis of atypical metastatic patterns.
Case Description/
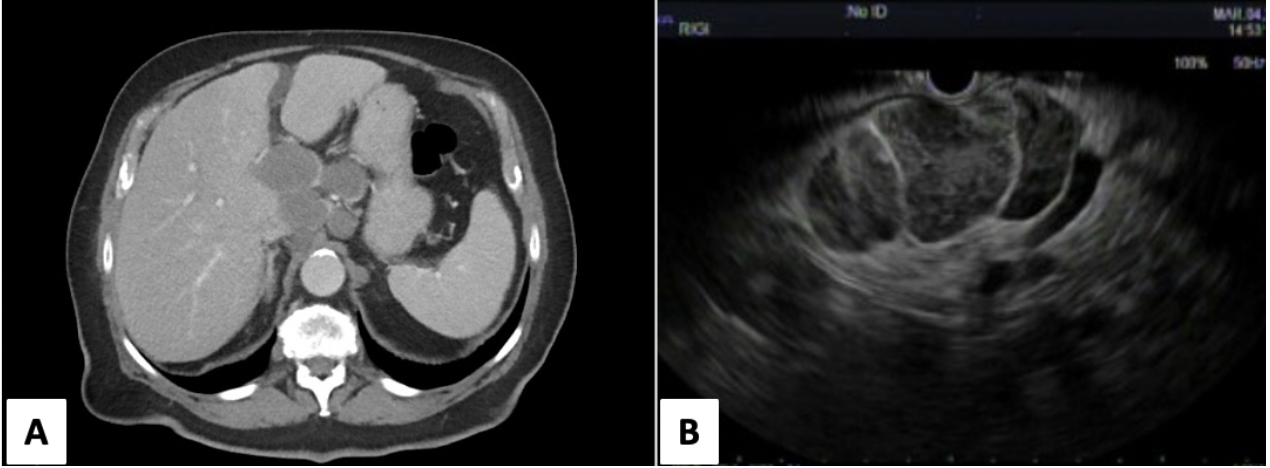
Methods: An 88-year-old male with a history of hypertension, coronary calcifications, gastroesophageal reflux disorder and EGJOO with prior dilations and botox injections presented with epigastric pain and worsening dysphagia. On presentation, his vitals were stable. Abdominal examination revealed tenderness in the epigastrium and right upper quadrant. Laboratory investigations were unremarkable. Computed tomography (CT) of abdomen and pelvis demonstrated multiple enlarged upper abdominal lymph nodes highly suspicious for malignancy. The patient was scheduled for esophagogastroduodenoscopy given his symptoms of dysphagia as well as endoscopic ultrasound (EUS) for further evaluation of abdominal lymphadenopathy. Biopsy of an abdominal lymph node from EUS demonstrated metastatic MCC with areas of necrosis. No primary skin lesion was identified. Discussion: In this case, the patient's initial symptoms were epigastric pain and dysphagia with later CT findings of multiple enlarged abdominal lymph nodes which is an unusual presentation for MCC. Although MCC frequently spreads to regional lymph nodes and distant organs, involvement of abdominal nodes without a known primary or with an obscure cutaneous lesion is rare. This atypical pattern highlights the importance of maintaining a broad differential diagnosis and consideration of occult malignancy evaluation when evaluating unexplained abdominal symptoms and EGJOO. This case demonstrates the utility of EUS-guided fine needle aspiration in making tissue diagnosis and serves as a reminder of the diverse metastatic pathways of MCC and the need for clinicians to consider it in the differential diagnosis of deep-seated lymphadenopathy.
Figure: Figure 1. A. CT Abdomen demonstrating upper abdominal lymphadenopathy. B. EUS with demonstration of large celiac axis lymph nodes measuring up to 4 x 6 cm used for fine needle aspiration.
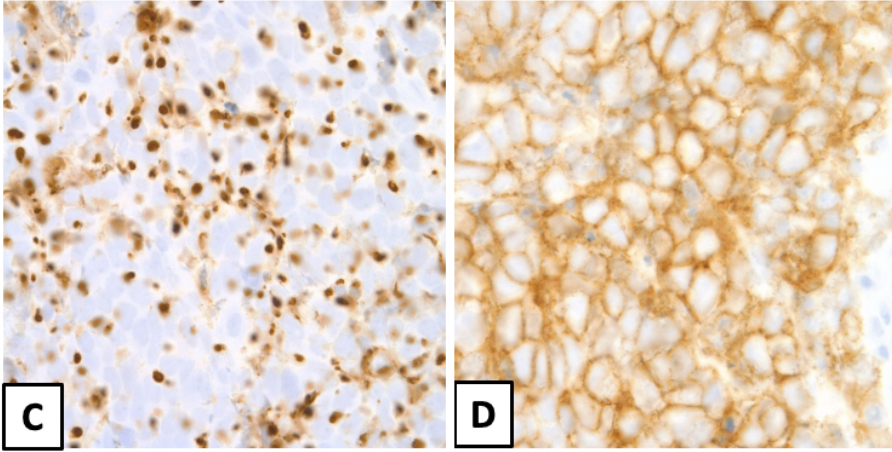
Figure: Figure 2. C. Immunohistochemical stain positive for cytokeratin 20. D. Immunohistochemical stain positive for CD56.
Disclosures: Andrew Petrou indicated no relevant financial relationships. Alex Chang indicated no relevant financial relationships. Priya Kumari Maheshwari indicated no relevant financial relationships. Li Wang indicated no relevant financial relationships.
Andrew L. Petrou, MD1, Alex Chang, MD1, Priya Kumari Maheshwari, MD2, Li Wang, MD1. P5146 - An Unexpected Culprit: Epigastric Pain Unveiling Merkel Cell Carcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")