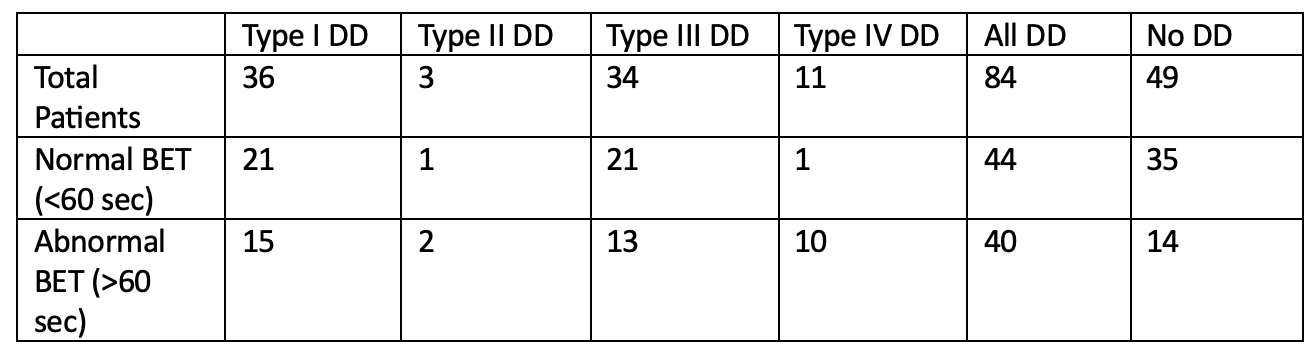
Jason Goldenberg, MD1, Zachary Wilmer Reichenbach, MD, PhD2, Henry P.. Parkman, MD, FACG2 1Temple University, Philadelphia, PA; 2Temple University Hospital, Philadelphia, PA Introduction: The London Protocol (LP) for characterization and classification of anorectal (AR) function requires the utilization of a balloon expulsion test (BET) (or defecography) in conjunction with anorectal manometry (ARM). ARM alone has shown to poorly differentiate between healthy volunteers and patients with functional constipation. Performing BET alone has been suggested to screen for AR disfunction without need for diagnostic ARM. We set out to determine the relationship of ARM and BET testing for AR dysfunction as well as predictors for abnormal BET. We then evaluated patients who completed biofeedback therapy (BFT) to assess response. Methods: We analyzed 133 ARM studies performed using a modified LP on patients presenting for constipation. ARM was performed using high resolution anal manometry (Manoscan AR High Resolution Manometry System, Minneapolis MN). BET with a rectal balloon filled with 50 cc of water was performed immediately following ARM. Patients were analyzed based on ARM pattern and BET. Results: Of 133 patients, 54 (40.6%) patients had prolonged BET. 84 (63.1%) patients had ARM evidence of dyssynergic defecation (DD). Of these 84 patients, 40 (48%) had an abnormal BET ( >60 sec). Of 49 patients without DD, 14 (29%) had an abnormal BET. Although there was a significant relationship between ARM and BET (p=0.03), BET had poor sensitivity and specificity to ARM findings (52.4% and 28.6% respectively). We assessed manometric predictors of abnormal BET. Poor intrarectal force during simulated defecation was significantly associated with abnormal BET (< 50 mmHg vs >50 mmHg; p=0.023). There was no significant relationship between anal sphincter relaxation and abnormal BET (68% of patients with >20% AR had a normal BET and 55% with < 20% AR had a normal BET; p=0.14). Patients having either Type I or III DD were significantly more likely to have normal BET compared to type II or IV (p=0.002). 21 patients from this cohort underwent BFT. Symptomatic improvement was seen in 5 (83%) patients with both tests abnormal, 13 (93%) patients with abnormal manometry, and in the 1 patient with only an abnormal BET. Discussion: ARM and BET are both important metrics for determining disorders of AR muscular coordination. Patients with either test abnormal benefit from BFT. Evaluating for AR dysfunction without including ARM will miss a significant portion of patients who may benefit from BFT. The combination of these tests when combined with clinical symptoms should be used to determine treatment.
Figure: Table 1: Normal vs. Abnormal Balloon Expulsion Tests by Subtype of Dyssynergic Defecation
Disclosures: Jason Goldenberg indicated no relevant financial relationships. Zachary Wilmer Reichenbach indicated no relevant financial relationships. Henry Parkman indicated no relevant financial relationships.
Jason Goldenberg, MD1, Zachary Wilmer Reichenbach, MD, PhD2, Henry P.. Parkman, MD, FACG2. P5069 - Use of Anorectal Manometry and Balloon Expulsion Testing to Assess Anorectal Dysfunction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.