Mohammed Z. Rehman, MD1, Mariya Syed, MD1, Mohammed A. Ahmed, MBBS2, Shane Quo, DO3, Alexander Davis, DO3, Dilip Ghanekar, MD3 1HCA Florida Healthcare, Land O Lakes, FL; 2Deccan College of Medical Sciences, Hyderabad, Telangana, India; 3HCA Florida Healthcare, Hudson, FL Introduction: Esophageal candidiasis (EC) remains the most common cause of infectious esophagitis, predominantly affecting the immunocompromised. It typically presents with odynophagia, dysphagia, and retrosternal discomfort, and progression to esophageal stricture formation is rare. Here, we report a case of EC leading to symptomatic esophageal strictures in a patient without overt immunosuppression
Case Description/
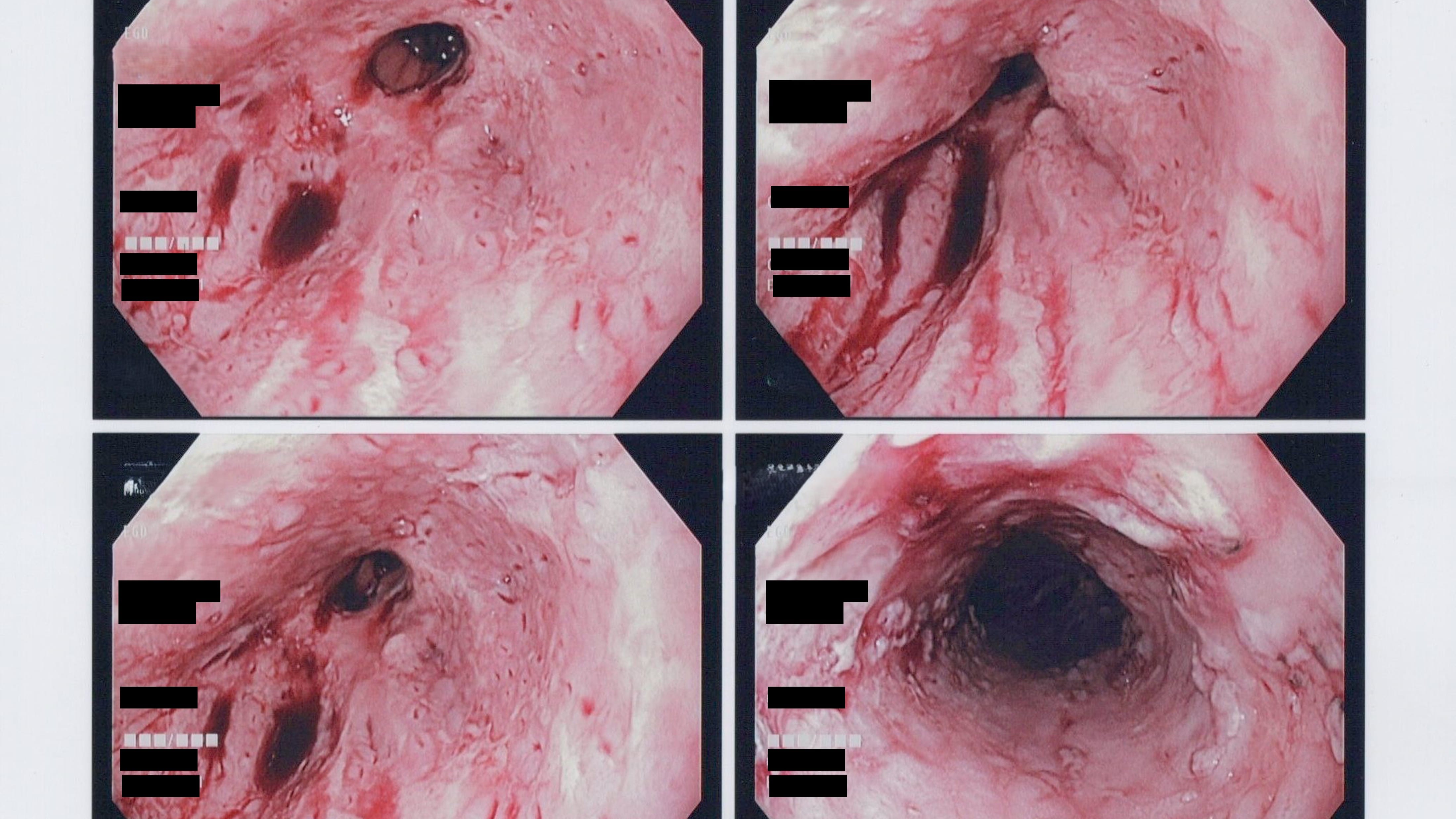
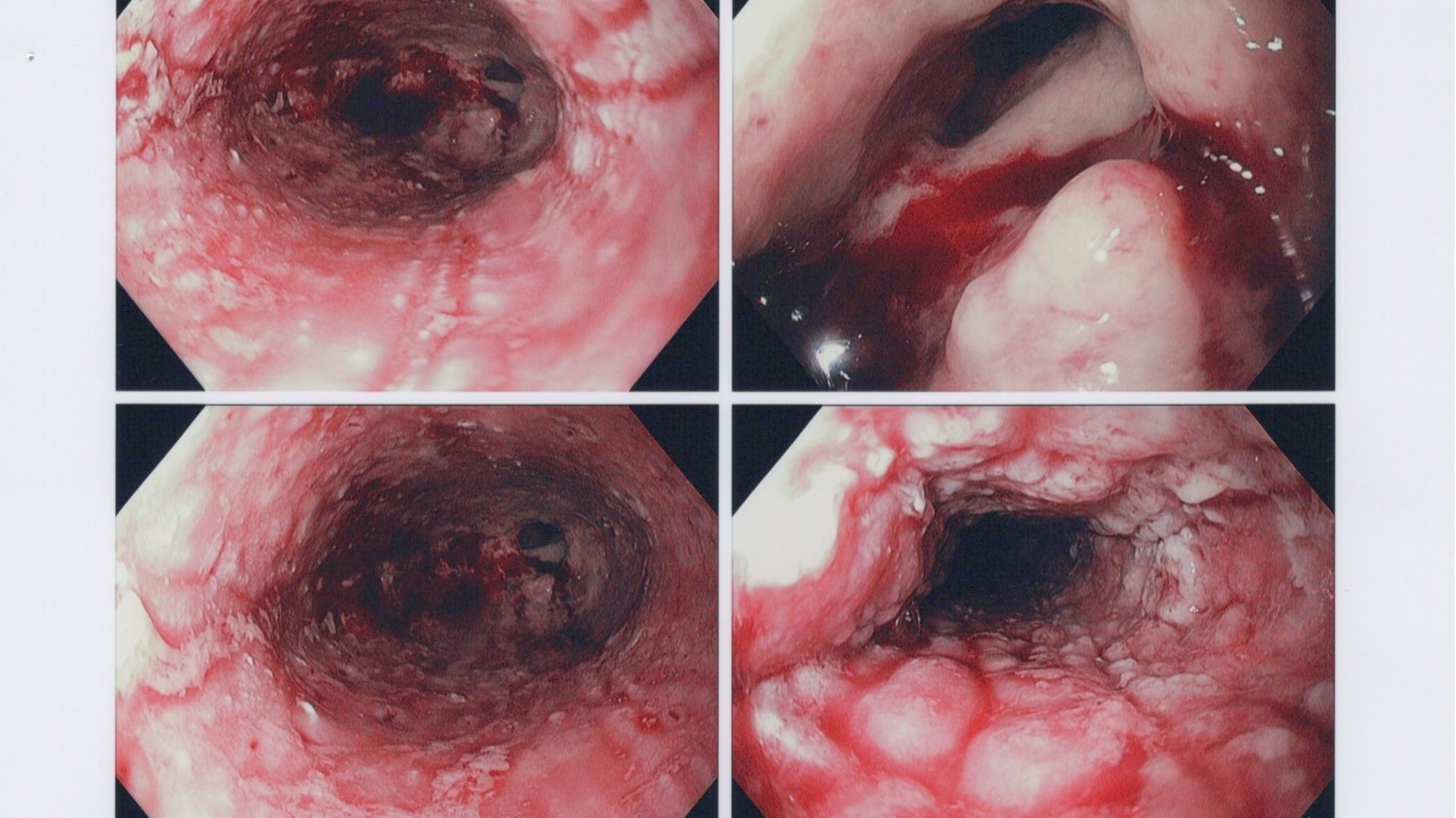
Methods: 68-year-old male with significant alcohol use disorder and known recurrent EC came with dysphagia, odynophagia, and coffee-ground emesis. He described pain and difficulty swallowing both solids and liquids, for the past few months. Vital signs were stable, and hemoglobin was low but stable at around 9g/dL. His serum alcohol level on admission was significantly elevated at 200 mg/dL. He underwent an EGD that showed extensive candidiasis and both proximal and distal esophageal strictures (Image 1A and 1B), which were dilated using a balloon up to 15mm. On further review of his medical chart, it was found that he recently had an EGD outpatient with balloon dilation for the same esophageal stricture. The patient was started on IV Fluconazole, and an HIV test performed was negative. The patient reported significant improvement in his symptoms after the esophageal dilation. The patient was discharged home with oral Fluconazole and was asked to follow up as an outpatient Discussion: EC is an opportunistic infection, affecting individuals with HIV/AIDS, malignancies, diabetes mellitus, or on immunosuppressants. In this patient, chronic alcohol likely played a contributing role. Several smaller studies and case reports suggest that chronic alcohol consumption can predispose individuals to Candida infections even in the absence of overt immunosuppression. A rare complication was the development of a proximal and distal esophageal strictures. Importantly, no alternate causes of stricture, such as GERD, medication-induced injury, or caustic ingestion, were identified in this patient. Less common complications of EC include ulceration (seen in our patient), intramural pseudo-diverticulosis, and hyperkeratosis, which may predispose to perforation or fistula formation.
This case emphasizes that EC, while uncommon in immunocompetent individuals, can still occur and lead to complications such as esophageal strictures. Chronic alcoholism may act as a contributing factor. Early recognition and a combined approach involving antifungal therapy and endoscopic dilatation may be necessary for optimal management
Figure: EGD showing White plaques, ulcerations and strictures
Figure: EGD showing White plaques, ulcerations and strictures
Disclosures: Mohammed Rehman indicated no relevant financial relationships. Mariya Syed indicated no relevant financial relationships. Mohammed Ahmed indicated no relevant financial relationships. Shane Quo indicated no relevant financial relationships. Alexander Davis indicated no relevant financial relationships. Dilip Ghanekar indicated no relevant financial relationships.
Mohammed Z. Rehman, MD1, Mariya Syed, MD1, Mohammed A. Ahmed, MBBS2, Shane Quo, DO3, Alexander Davis, DO3, Dilip Ghanekar, MD3. P5055 - Beyond Immunosuppression: Recurrent Esophageal Candidiasis and Stricture Formation in a Patient With Chronic Alcohol Use, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.