Juan G. Feliciano-Figueroa, MD, Alondra Velez-Santiago, MD, Priscilla Magno-Pagatzaurtundua, MD, MSc VA Caribbean Healthcare System, San Juan, Puerto Rico Introduction: Dysphagia is a common gastrointestinal symptom that may reflect benign and malignant underlying diseases. While esophageal cancer is often a primary concern, rare infectious causes must also be considered in patients with relevant environmental exposures. This case highlights an unusual presentation of endemic fungus with progressive dysphagia as the primary symptom, mimicking a malignancy and underscoring the need of multidisciplinary diagnostic approach while evaluating dysphagia.
Case Description/
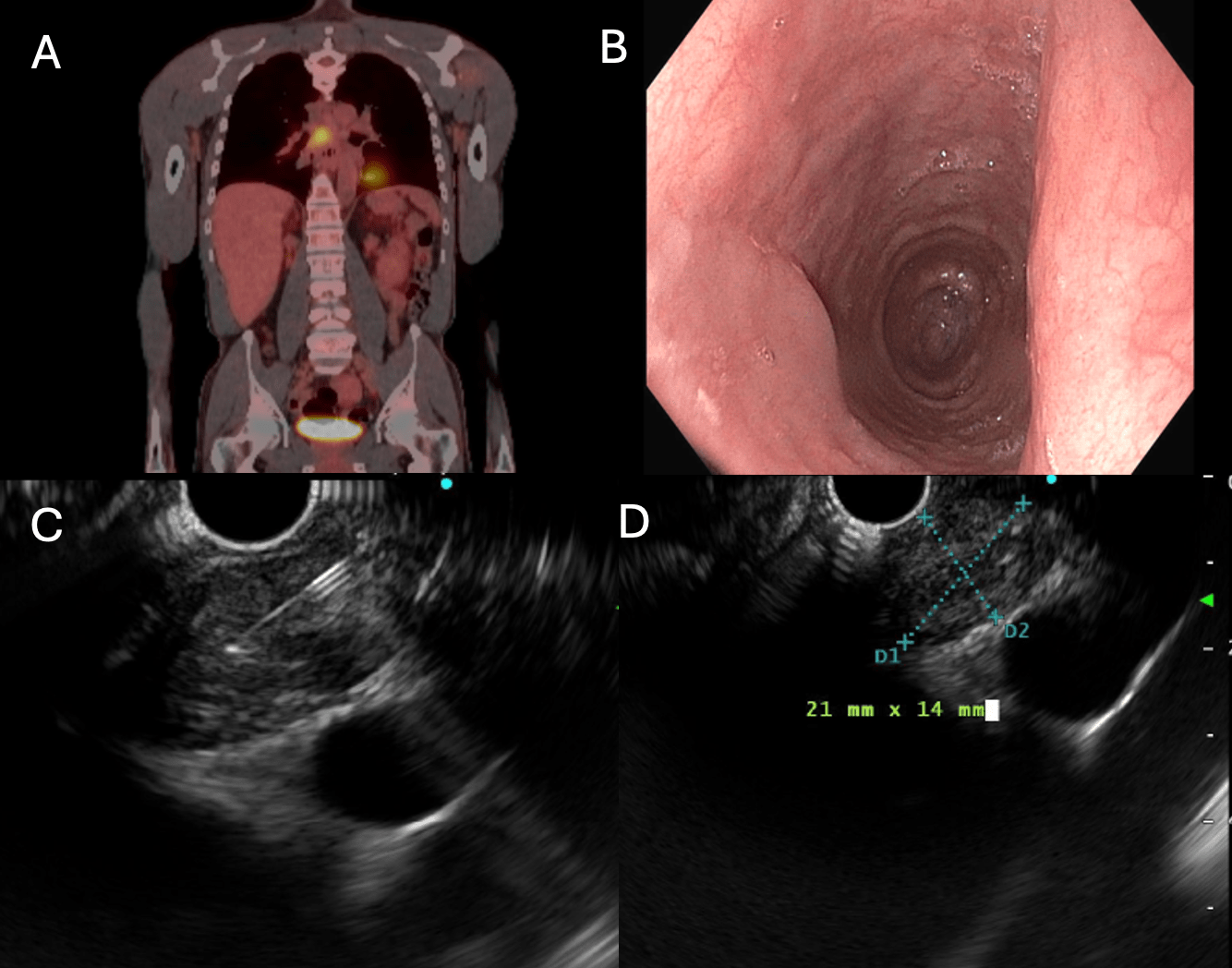
Methods: A 53-year-old male with medical history of 30-pack-year smoking and prior alcohol abuse presented with progressive dysphagia to solids and need for water to pass bolus. Also reported weight loss, intermittent fevers, fatigue and exertional dyspnea over the last year. A chest CT revealed a mass-like lesion near the esophagus, measuring up to 4.5 cm in diameter. PET scan showed hypermetabolic activity on the subcarinal compartment of the mediastinum, raising suspicion for malignancy. An endoscopy was done and did not identify any type of mass within the esophagus. An EUS was performed with a double setup along with EBUS. A biopsy was taken from the mass using EUS, and mediastinal lymph nodes were biopsied via EBUS (stations 7 and 11R/L). Both biopsies revealed granulomatous lymphadenitis. Gram stain, special stains, and cultures were negative for bacteria, fungi, and tuberculosis. Due to patient’s history of deployment to dusty environments in Fort Bliss and El Paso Texas, a fungal panel was ordered. Coccidioides serologies reported serum IgG titers 1:32. Since symptoms were present, the patient was treated with fluconazole for seven months, leading to resolution of the mass on follow-up CT. The patient reported compliance with antifungal therapy and resolution of symptoms. Discussion: This report presents a rare progressive dysphagia due to extrinsic esophageal compression from a mediastinal mass caused by Coccidioidomycosis, which typically presents as pulmonary infection but can manifest atypically. One such presentation is the formation of a mediastinal mass due to granulomatous inflammation, which closely mimics malignancy on imaging. In this case the absence of malignancy on repeated biopsy and the eventual identification of granulomatous inflammation raised suspicion for an infectious cause. Fungal serologies were then pursued and confirmed the diagnosis. Maintaining a broad differential in cases of unexplained dysphagia and mediastinal pathology avoids unnecessary procedures.
Figure: A. PET scan B. Upper Endoscopy - mid esophagus. No evidence of epithelial or subepithelial abnormalities C and D. Endoscopic Ultrasound (EUS)
Disclosures: Juan G. Feliciano-Figueroa indicated no relevant financial relationships. Alondra Velez-Santiago indicated no relevant financial relationships. Priscilla Magno-Pagatzaurtundua indicated no relevant financial relationships.
Juan G. Feliciano-Figueroa, MD, Alondra Velez-Santiago, MD, Priscilla Magno-Pagatzaurtundua, MD, MSc. P5054 - Fungus Among Us: A Rare Cause of Dysphagia, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.