Mina Awadallah, MD, MSc1, Seema R. Gandhi, MD2, Vikram Kotwal, MD3, John Erikson Yap, MD, MBA, FACG4 1University of Utah, Salt Lake City, UT; 2Cook County Health, Chicago, IL; 3John H. Stroger, Jr. Hospital of Cook County, Chicago, IL; 4University of Utah Health, Salt Lake City, UT Introduction: Esophageal diverticula are rare structural outpouchings of the esophageal wall, with a prevalence of less than 1% in the general population. These lesions result from a weakness in the esophageal wall and are categorized by anatomical location into Zenker’s (pharyngoesophageal), mid-esophageal, and epiphrenic (distal esophageal) types. Mid-esophageal diverticula are particularly uncommon and are most often associated with underlying esophageal motility disorders or traction from chronic mediastinal inflammation or fibrosis. While many cases are incidental findings, larger or poorly draining diverticula can present with dysphagia, regurgitation, halitosis, or aspiration. We present a case of a large symptomatic mid-esophageal diverticulum in the absence of any detectable motility abnormality.
Case Description/
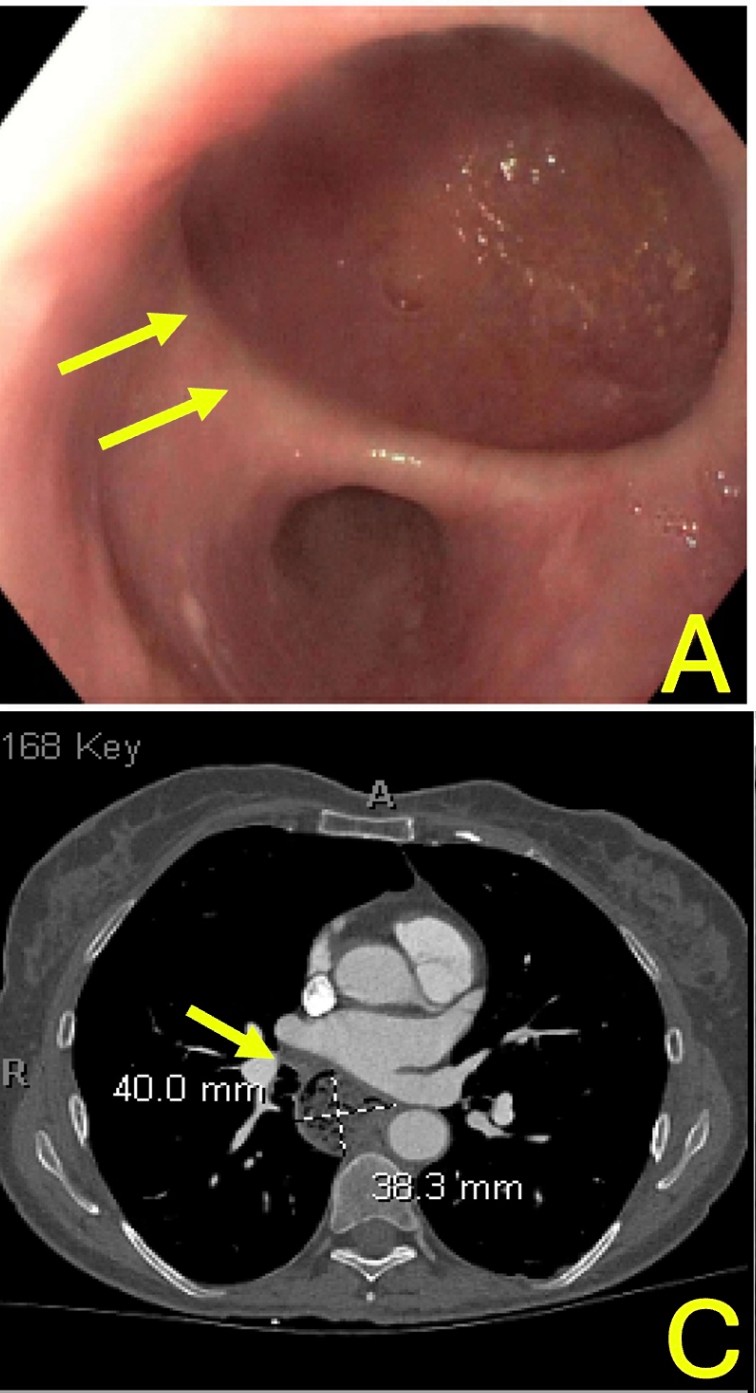
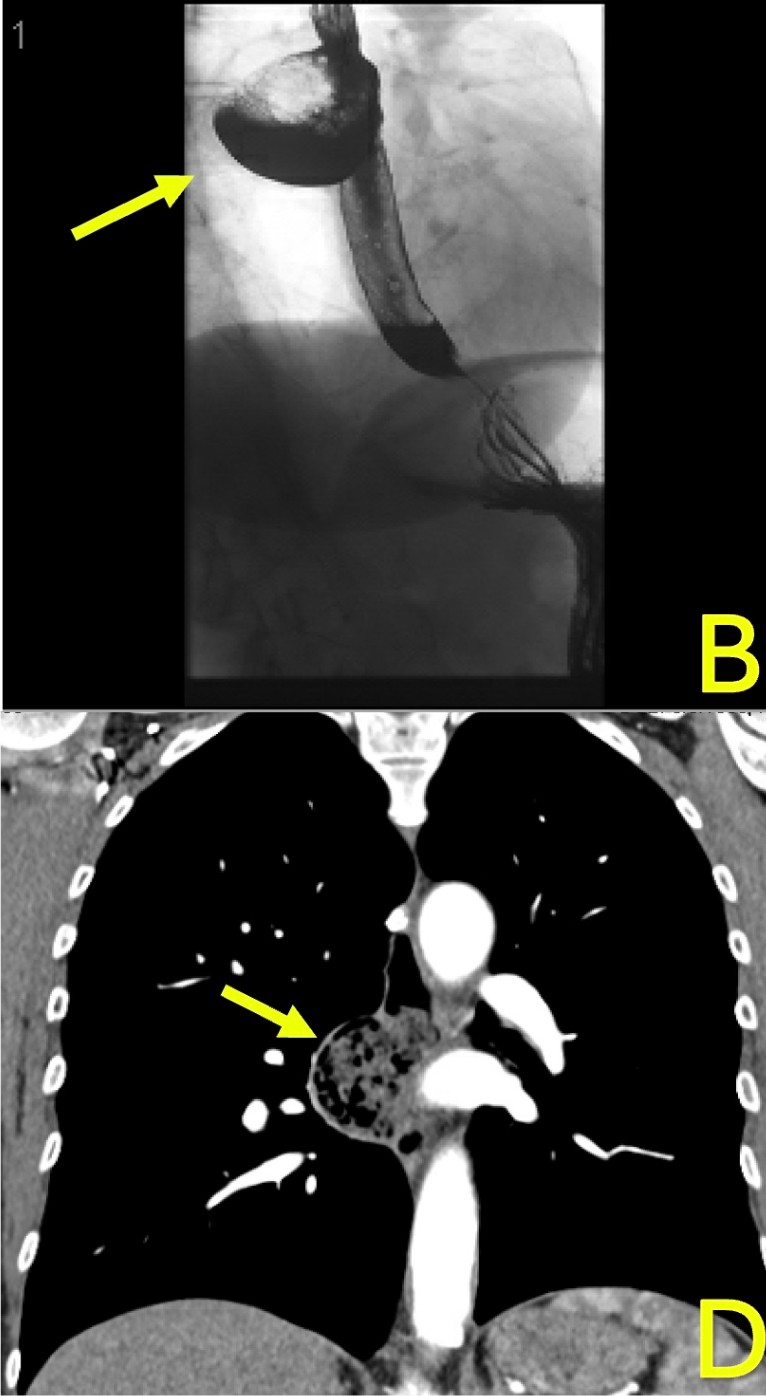
Methods: A 65-year-old woman was referred for several months of progressive dysphagia to both solids and liquids, without associated odynophagia, weight loss, or gastroesophageal reflux symptoms. Esophagogastroduodenoscopy (EGD) revealed a large mid-esophageal diverticulum with otherwise normal-appearing mucosa. No strictures, ulcers, or masses were seen. A small sliding hiatal hernia was identified. Biopsies obtained from the mid and distal esophagus were unremarkable and demonstrated no evidence of eosinophilic esophagitis or other inflammatory pathology. Barium esophagram revealed a right-sided, laterally projecting diverticulum measuring 3.3 x 4.7 cm with a 2.5 cm neck. Chest CT confirmed the presence of the diverticulum containing retained food material, with no surrounding lymphadenopathy or evidence of mass effect. High-resolution esophageal manometry demonstrated intact primary peristalsis and normal lower esophageal sphincter relaxation, effectively excluding motility disorders such as achalasia or spasm. Given her ongoing symptoms and radiologic findings, the patient was referred for surgical evaluation. Discussion: Mid-esophageal diverticula are typically linked to underlying motility disturbances or traction from mediastinal pathology. However, this case highlights a structural cause of dysphagia in a patient with normal manometry. Retained food and impaired emptying of the diverticulum support a mechanical etiology. Evaluation using endoscopy, barium esophagram, cross-sectional imaging, and manometry can help guide appropriate management. Surgical management is warranted in symptomatic patients with significant anatomical findings.
Figure: A. Endoscopic view of a mid-esophageal diverticulum. C. CT images revealing a mid-esophageal diverticulum containing retained food material.
Figure: B. Barium esophagram demonstrating contrast pooling within the diverticular pouch. D. CT images revealing a mid-esophageal diverticulum containing retained food material.
Disclosures: Mina Awadallah indicated no relevant financial relationships. Seema Gandhi indicated no relevant financial relationships. Vikram Kotwal indicated no relevant financial relationships. John Erikson Yap: Phathom Pharmaceutical – Speakers Bureau. Steris – Consultant.
Mina Awadallah, MD, MSc1, Seema R. Gandhi, MD2, Vikram Kotwal, MD3, John Erikson Yap, MD, MBA, FACG4. P5052 - Caught in the Pouch: A Rare Case of Dysphagia Without Dysmotility, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.