Sanitha Pulapattassery, MD, Omowonuolaoluwa Adebari, MD, Sharathi Sirimanne, MD, Mohankumar Doraiswamy, MD Mercy Hospital Fort Smith, Fort Smith, AR Introduction: Black pleural effusion (BPE) is a very rare condition with only a handful number of cases described in the literature. Causes include malignant melanoma, pancreaticopleural fistula with pseudocyst, lung adenocarcinoma and atypical fungal infections. We describe a case of a black pleural effusion that was positive for Aspergillus Niger and enteric organisms following Boerhaave syndrome.
Case Description/
Methods: A 65 year old male with past medical history significant for gastroesophageal reflux disease presented to the emergency department (ED) with sudden onset of shortness of breath, epigastric abdominal pain and intractable vomiting. He was working on his unfinished old basement for the past 2 years and has been experiencing some cough and congestion intermittently especially on the days he worked in the basement where he had noticed black mold before. In the ED, he was tachycardic and hypoxic requiring noninvasive pressure ventilation requiring admission to the ICU. Labs include leukocytosis of 15,200/uL with predominant neutrophilia, but blood cultures were negative. Computerized Tomography Angiography (CTA) of chest, abdomen and pelvis revealed a moderate to large right-sided pleural effusion with worsening pneumothorax requiring chest tube placement. Chest tube drained black colored pleural fluid. Voriconazole was added due to suspicion of a fungal infection. The following day, pleural fluid turned clear with cultures growing Enterococcus faecalis, Lactobacillus, Candida albicans and Aspergillus fumigatus. Pleural fluid studies suggested exudative effusion with elevated amylase level of 4281U/L but negative for malignant cells. Repeat CT chest abdomen with oral contrast revealed extravasation of oral contrast into the right pleural effusion consistent with gastroesophageal perforation near the posterior GE junction. Subsequently, he underwent right thoracotomy and repair of esophageal perforation and decortication of right lung requiring intubation. Respiratory status improved and CT confirmed no extravasation of contrast. Barium swallow study was negative for residual GE leak. He was discharged on antibiotics with outpatient ID follow up. Discussion: This case aims to add to the existing literature and increase awareness of this rare condition with Boerhaave syndrome as an important differential diagnosis for BPE. Treatment of the underlying cause is crucial for a favorable outcome. Early diagnosis has improved outcomes through prompt initiation of treatment.
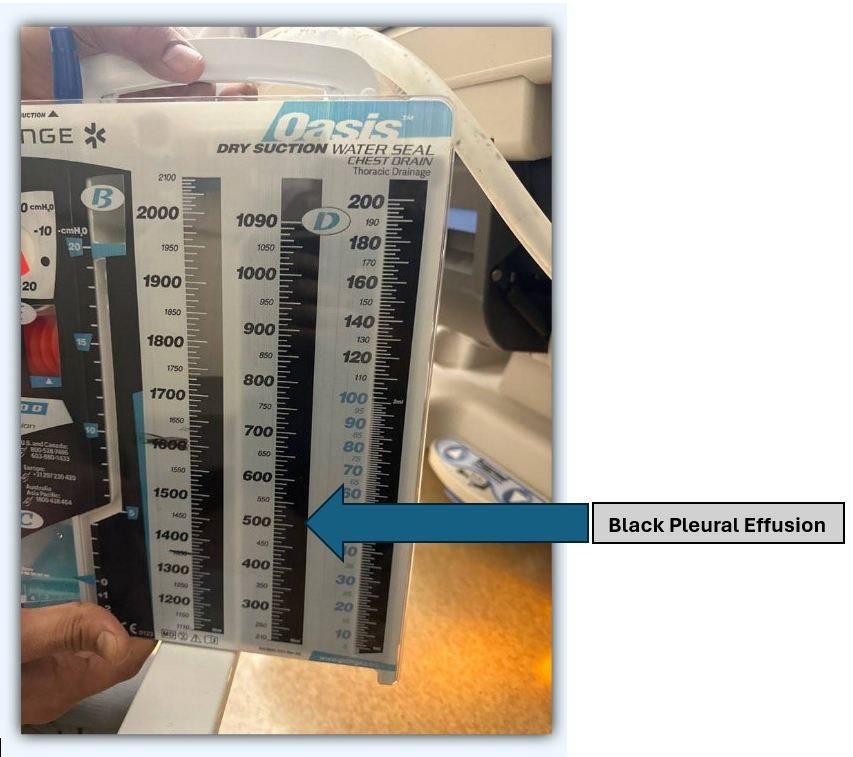
Figure: Black Pleural Effusion
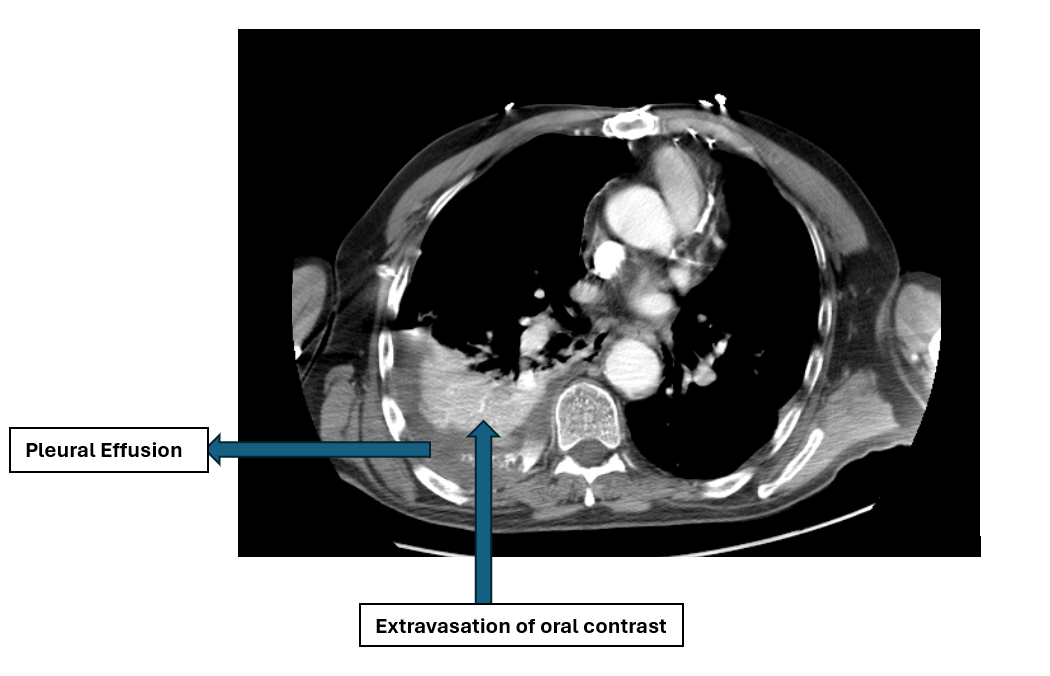
Figure: CT chest with extravasation of oral contrast and pleural effusion
Disclosures: Sanitha Pulapattassery indicated no relevant financial relationships. Omowonuolaoluwa Adebari indicated no relevant financial relationships. Sharathi Sirimanne indicated no relevant financial relationships. Mohankumar Doraiswamy indicated no relevant financial relationships.
Sanitha Pulapattassery, MD, Omowonuolaoluwa Adebari, MD, Sharathi Sirimanne, MD, Mohankumar Doraiswamy, MD. P5013 - A Rare Case of Black Pleural Effusion: Boerhaave Syndrome With Pulmonary Aspergillosis in Immunocompetent, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.