Meghana Vankina, MD1, Jayaprakash Sreenarasimhaiah, MD, FACG2 1Tulane School of Medicine, New Orleans, LA; 2Baylor Scott & White Medical Center Irving, Dallas, TX Introduction: Giant fibrovascular esophageal polyps are rare, benign tumors but their size and vascularity often lead to referral for surgical resection1. However, with early gastroenterology involvement and careful patient evaluation, a minimally invasive endoscopic approach is possible. This case demonstrates how multidisciplinary collaboration helped avoid thoracic surgery in a patient referred for operative management and led to excellent long-term outcomes.
Case Description/
Methods: A 60-year-old male was referred to thoracic surgery after evaluation by his primary care physician for persistent sore throat, regurgitation, fever, and night sweats. Computed tomography (CT) revealed a large intraluminal esophageal mass extending from the cervical esophagus toward the gastroesophageal junction. Though the patient denied classic dysphagia, he has had intermittent difficulty swallowing water and had been choking on rice. Upper endoscopy confirmed a large, likely fibrovascular polyp; however biopsy was deferred due to bleeding risk.
Open resection was initially considered, but gastroenterology was consulted to determine whether a more minimally invasive approach was possible. After multidisciplinary discussion, the patient underwent transoral resection using a combined rigid and flexible endoscopic technique with snare polypectomy. A 20 cm fibrovascular polyp was removed in two stages: a 5x15 cm segment followed by a 5x5 cm mass. The patient recovered well and was asymptomatic at his 3-week follow-up.
Three years later, the patient presented with mild dysphagia. Repeat endoscopy revealed scar tissue and a cricopharyngeal web at the prior resection site, which were successfully treated with balloon dilation. No recurrence of the polyp was found. Discussion: This case demonstrates how early gastroenterology involvement and multidisciplinary planning can allow for successful endoscopic resection of giant esophageal polyps that are traditionally managed with surgery. The patient avoided a thoracotomy and experienced 3 years of symptom relief. When the symptoms returned, they were due to post-resection scarring and managed endoscopically. This case supports minimally invasive treatment as a viable, long-lasting option for complex esophageal lesions and highlights the importance of multidisciplinary care.
References:
Ward MA, Beard KW, Teitelbaum EN, et al. Endoscopic resection of giant fibrovascular esophageal polyps. Surg Endosc. 2018;32(2):1066-1067. doi:10.1007/s00464-017-5664-0
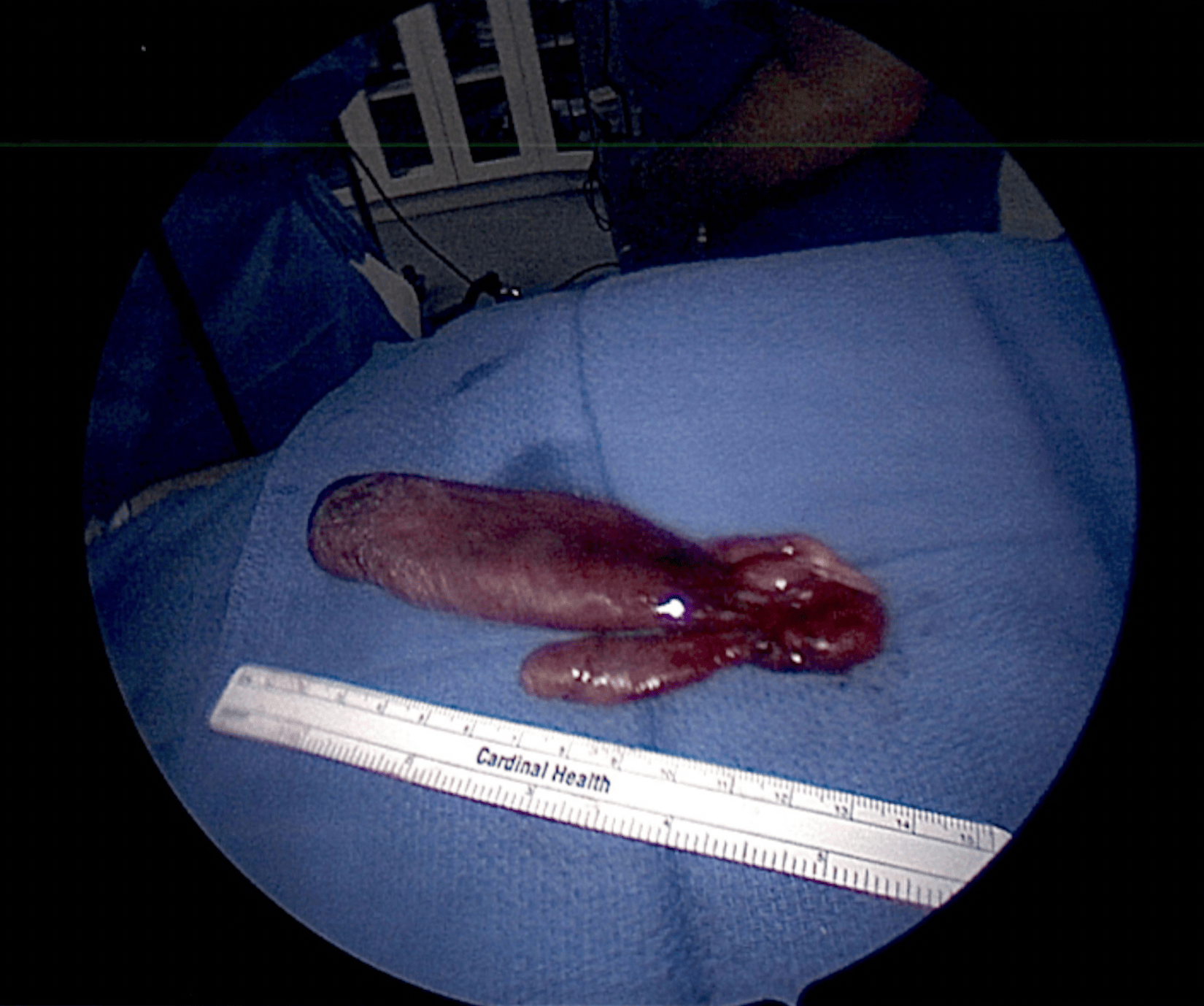
Figure: Gross specimen of a fibrovascular esophageal polyp segment resected endoscopically using a combined rigid and flexible approach. This represents one segment of the total polyp that measures approximately 20 cm in total length, originating at the cricopharyngeus and extending distally into the esophagus.
Disclosures: Meghana Vankina indicated no relevant financial relationships. Jayaprakash Sreenarasimhaiah indicated no relevant financial relationships.
Meghana Vankina, MD1, Jayaprakash Sreenarasimhaiah, MD, FACG2. P5012 - Endoscopic Resection of a Giant Fibrovascular Esophageal Polyp: A Minimally Invasive Alternative to Surgery, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.