University of Texas Health Science Center at San Antonio San Antonio, TX
Anudeeksha Satheeshkumar, MD1, Charles B. Miller, MD2 1University of Texas Health Science Center at San Antonio, San Antonio, TX; 2University of Texas Health San Antonio, San Antonio, TX Introduction: The presence of esophageal white plaques is a classic finding used to help diagnose Candida esophagitis. We present a case of an immunosuppressed patient with recurrent odynophagia and presence of esophageal white plaques on repeated endoscopy who received several empiric courses of treatment for Candida esophagitis before he was eventually diagnosed with mycophenolate mofetil-induced esophagitis.
Case Description/
Methods: A 55-year-old male with interstitial lung disease status-post bilateral lung transplant 5 months prior was evaluated for odynophagia. His medication regimen included tacrolimus, mycophenolate mofetil, and prednisone. Vitals were stable on admission, and physical exam was notable for thrush. Labs revealed neutropenia. Six weeks prior, the patient had undergone EGD for the same complaint, which revealed diffuse white plaques in the middle-third of the esophagus. Esophageal brushings had been collected, and he was treated empirically for suspected Candida esophagitis. Brushings returned without fungal elements. EGD from the current admission again showed circumferential white plaques, concerning for Candida esophagitis recurrence. The patient received empiric treatment with an extended course of fluconazole. However, biopsies returned without fungal organisms. He was re-admitted 1 week later for recurrent symptoms and underwent a third EGD, which showed a 3 cm area of denuded mucosa. Biopsies showed marked ulceration, but were negative for fungal elements or viral organisms. Though there are no pathognomonic or definitive pathologic findings of mycophenolate mofetil-induced esophagitis, his presentation and endoscopic findings were typical of this diagnosis. He presented 3 weeks later with severe dysphagia and was found to have a 5 cm by 6 mm mid-esophageal stenosis requiring 2 balloon dilations over the next 3 weeks. He has not required further evaluation over the past 6 months. Discussion: The presence of white plaques on endoscopic evaluation can be seen with many conditions, including esophageal leukoplakia secondary to chronic GERD, Candida esophagitis, medication-induced esophagitis, and EoE. Candida is the most common cause of infectious esophagitis. In a study, it was noted that gastroenterologists’ endoscopic suspicion of esophageal candidiasis was only accurate 46% of the time. Though infectious esophagitis will always be on the differential for dysphagia and odynophagia in those on immunosuppression, keep mycophenolate mofetil-induced esophagitis in your differential.
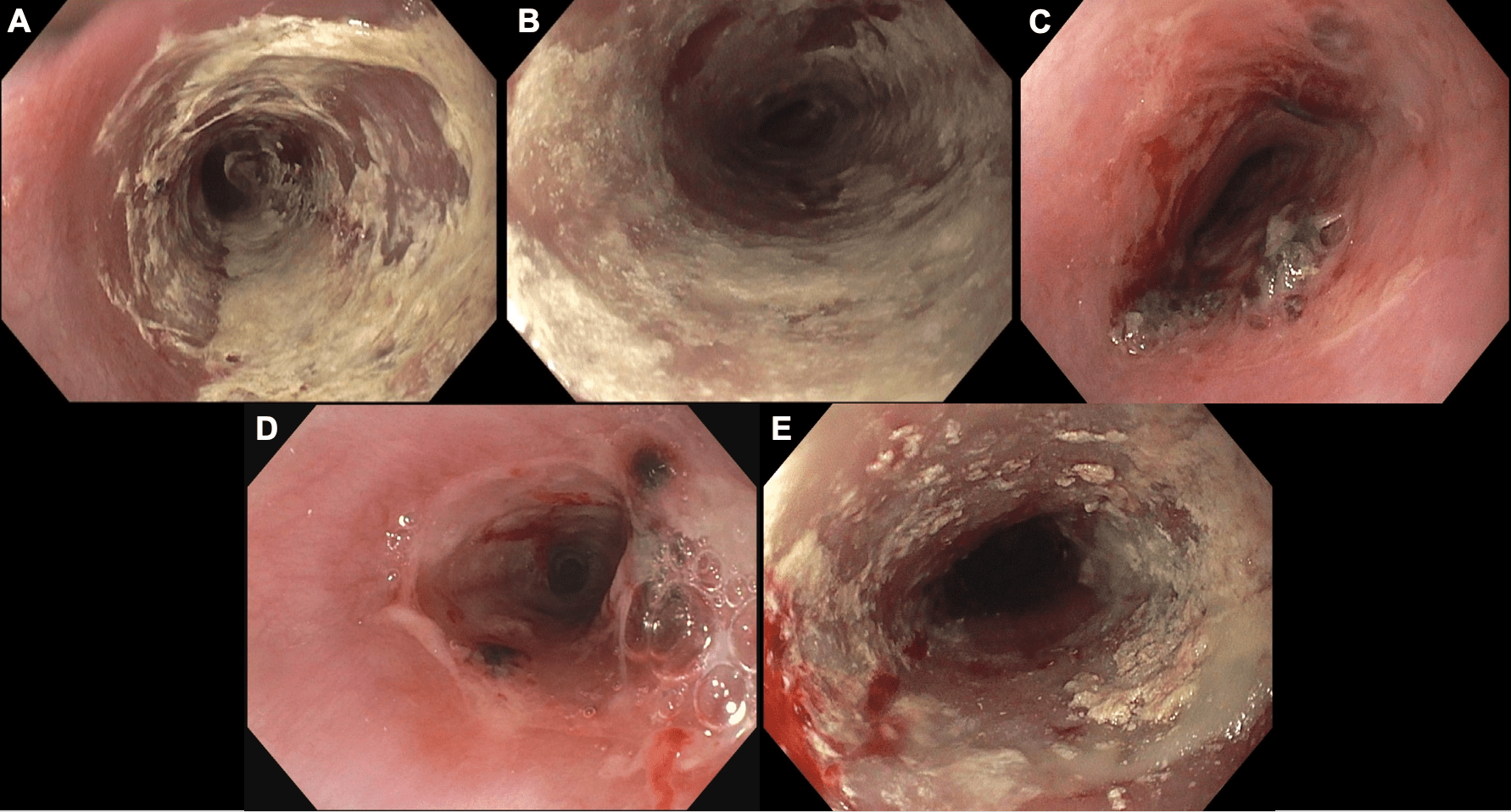
Figure: Panel A: 1st EGD for odynophagia, concern for Candida, brushed Panel B: 2nd EGD for odynophagia, concern for Candida, biopsied Panel C: 3rd EGD for odynophagia, no significant plaques, biopsied Panel D: 4th EGD for dysphagia, dilated to 12 mm Panel E: 5th EGD for dysphagia, dilated to 16.5 mm
Disclosures: Anudeeksha Satheeshkumar indicated no relevant financial relationships. Charles Miller indicated no relevant financial relationships.
Anudeeksha Satheeshkumar, MD1, Charles B. Miller, MD2. P5009 - Let's Be Candid: It's Not Always <i>Candida</i>, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")