Shaiv B. Patel, MD1, Anish V. Patel, MD2 1Mercy Health, Oklahoma City, OK; 2Robert Wood Johnson Medical School, Rutgers University, New Brunswick, NJ Introduction: “Downhill” esophageal varices (DEV) are dilated submucosal veins in the upper or mid esophagus in contrast to the more commonly found distal ("uphill") varices caused by portal hypertension. Common etiologies include superior venacava (SVC) obstruction related to mediastinal masses, fibrosing mediastinitis, and indwelling intravascular devices. Although rare, DEV may present with upper gastrointestinal bleeding.
Case Description/
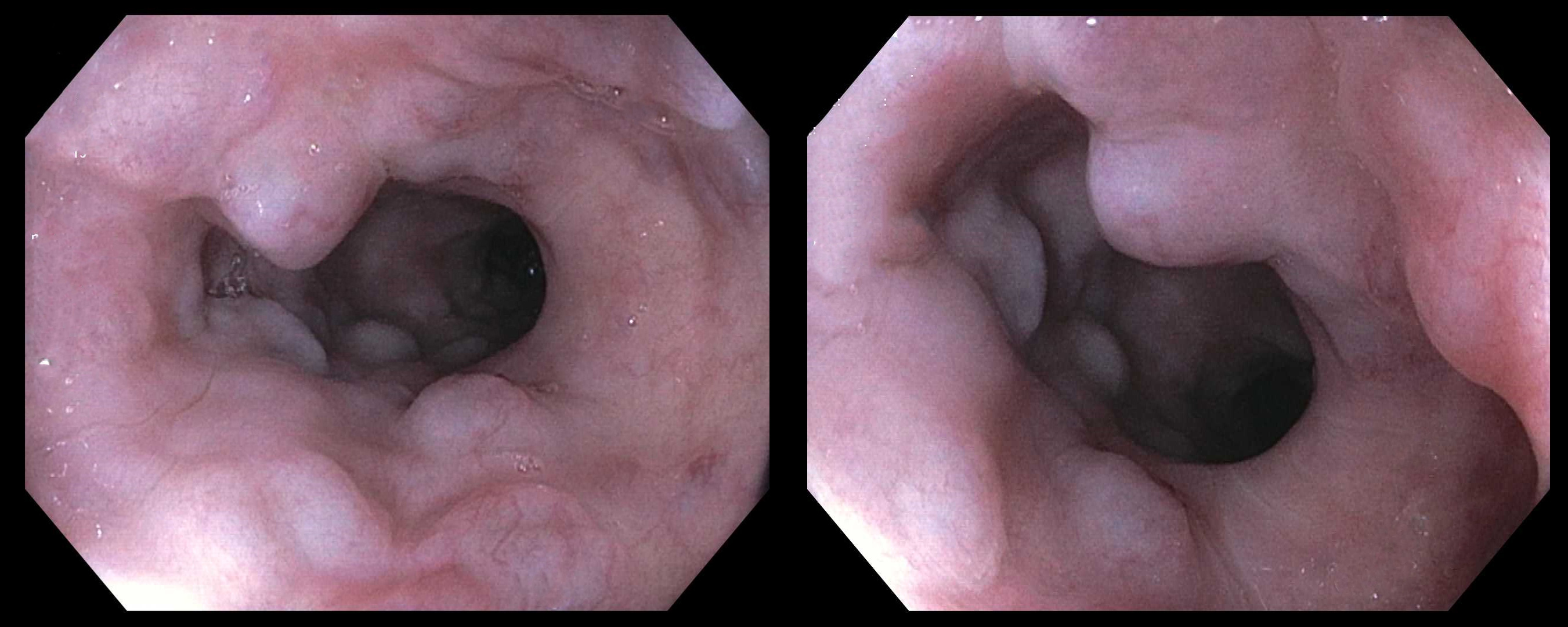
Methods: A 72 year-old Caucasian man with ischemic cardiomyopathy status post left ventricular assist device (LVAD) insertion, severe right ventricular dysfunction, moderate pulmonary hypertension and atrial fibrillation on warfarin therapy was referred for evaluation of iron deficiency anemia. He denied melena, hematochezia, hematemesis, abdominal pain or change in bowel habits. He has a history of small bowel angiectasias in the duodenum. Hemoglobin returned at 8.1 g/dL and iron saturation at 5%. He underwent a push enteroscopy that surprisingly revealed medium sized varices in the upper and mid esophagus with no stigmata of bleeding (Figure). A total of four nonbleeding angiectasias were identified in the proximal jejunum that were treated with argon plasma coagulation. CT chest and abdomen showed normal appearing liver, patent superior venacava, no ascites, and no mediastinal or lung masses. The LVAD was functional. The varices were attributed to his severe cardiac disease. Discussion: We present here a case of DEV related to advanced cardiomyopathy. DEV typically arising from SVC obstruction, can also result from functional impedance of venous return, as seen in patients with advanced cardiomyopathy. Elevated central venous pressure may lead to impaired SVC outflow and collateral venous circulation through the esophageal venous plexuses. Chronic venous congestion results in the development of DEV. Although less prone to hemorrhage than portal hypertensive varices, DEV varices can bleed, particularly in patients on anticoagulation or ventricular thromboembolism prophylaxis, common in the cardiomyopathy population. Endoscopically, these varices are confined to the upper or mid esophagus, sparing the distal esophagus, a key distinguishing feature. Recognition of DEV is critical in heart failure patients presenting with obscure or overt GI bleeding, especially when portal hypertension is absent. Management focuses on treating the underlying cardiac dysfunction or SVC obstruction, with endoscopic or interventional approaches reserved for active bleeding.
Figure: Striking finding of medium sized varices in the upper and mid esophagus on endoscopy.
Disclosures: Shaiv Patel indicated no relevant financial relationships. Anish Patel indicated no relevant financial relationships.
Shaiv B. Patel, MD1, Anish V. Patel, MD2. P5006 - Striking Finding of "Downhill" Esophageal Varices in an Individual With Advanced Cardiomyopathy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.