Tuesday Poster Session
Category: Esophagus
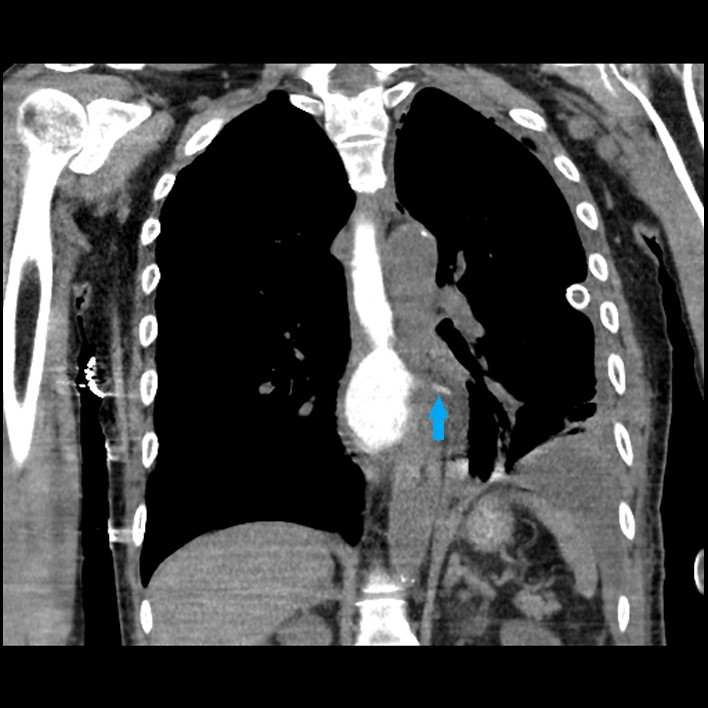
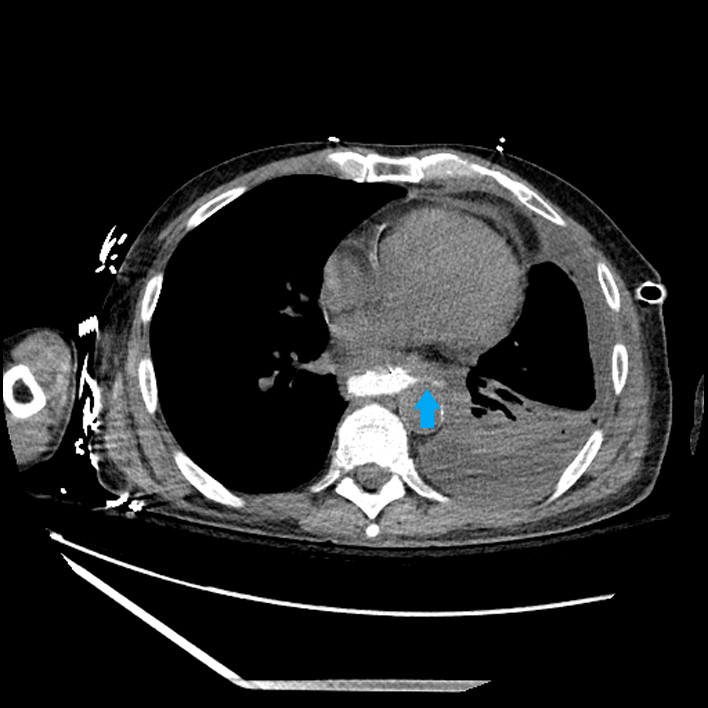
A Non-Stent Management of Esophageal Perforation Secondary to <i>Candida</i> Esophagitis Near the Gastroesophageal Junction
 photo")
Shyamal Sheth, DO (he/him/his)
Franciscan Health Olympia Fields
Chicago, IL