
Tuesday Poster Session
Category: Endoscopy Video Forum

Jeremy Polman, DO, MS, MBA
Lenox Hill Hospital, Northwell Health
New York, NY
A Roux-en-Y gastric bypass is an invasive procedure which involves surgically altering gastric anatomy typically for the purposes of weight loss through food restriction and malabsorption. During this procedure, a small gastric pouch is created from the stomach, which is then attached to a portion of the jejunum. The bypassed stomach and duodenum remain intact while the duodenal outflow is attached to a more distal portion of the jejunum. Complications after this procedure are uncommon, but typically include stenosis, ulceration, and bleeding. Here, we present a case involving the use of an endoscopic stent to recreate a stenosed gastro-jejunal anastomosis and bypass a gastro-gastric fistula.
Case Description/
Methods:
A 72-year-old female presented to the Emergency Department with unintentional weight loss of approximately 20 pounds, nausea and vomiting with oral intake of solids and liquids, and diffuse abdominal pain over the previous month. Surgical history includes Roux-en-Y gastric bypass more than 30 years prior, which was obtained for weight loss. CT abdomen and pelvis with oral contrast obtained at time of presentation identified narrowing of the gastro-jejunal anastomosis as well as oral contrast in the gastric remnant, concerning for gastro-gastric fistula. An EGD was performed the following day. Upon advancement of the gastroscope distal to the gastric pouch outlet, intubation of the bypassed remnant stomach through the gastro-gastric fistula was performed. The gastroscope was then withdrawn and maneuvered into the area of the gastro-jejunal anastomosis where a stricture was identified, which was unable to be traversed. Under fluoroscopic guidance, a guidewire was fed through the gastro-jejunal stricture into the jejunum. A covered 15 x 10mm endoscopic stent was then advanced over the guidewire until the midpoint of the stent deployment device was located at the midpoint of the gastro-jejunal stricture. The stent was successfully deployed and location was confirmed via fluoroscopy. The gastroscope was able to visualize jejunum distal the the stent, again confirming successful deployment, recreation of the gastro-jejunal anastomosis, and exclusion of the gastro-gastric fistula. Prior to discharge, the patient was able to advance diet and tolerated up to a puree diet without nausea or vomiting.
Discussion:
This unique case outlines an uncommon Roux-en-Y complication and a successful endoscopic therapy, which improved the patient’s symptoms and avoided requiring a surgical intervention. 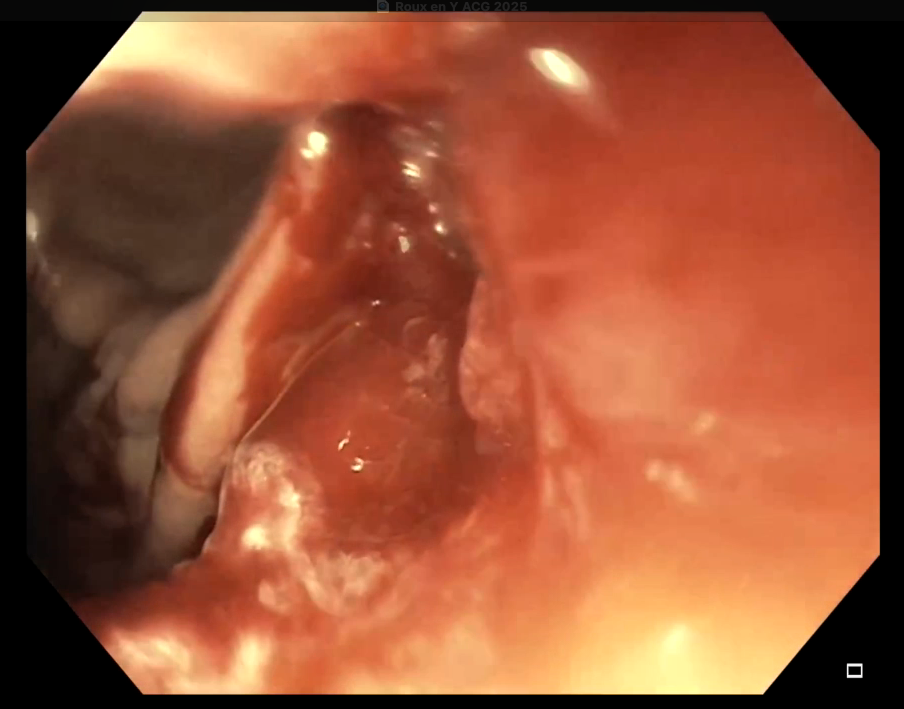
Figure: Endoscopic view from gastric pouch outlet. The gastro-gastric fistula is seen on the left side of the image. The strictured gastro-jejunal anastomosis is seen in the center of the image. 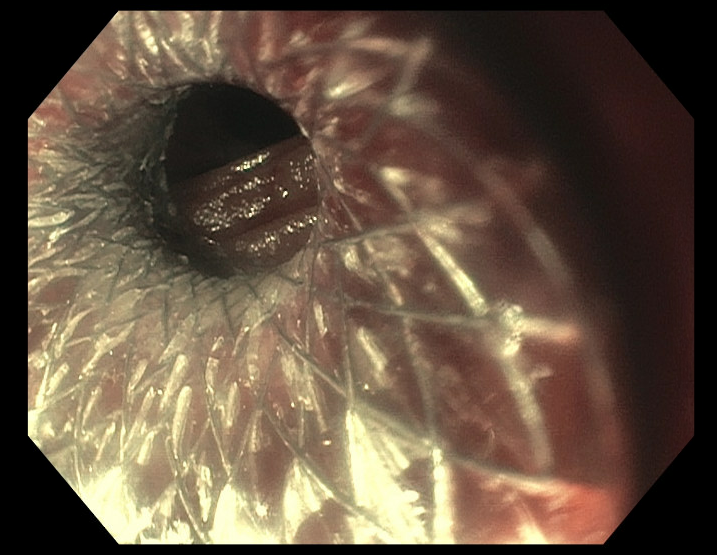
Figure: Endoscopic view of the endoscopically placed covered stent across the gastro-jejunal anastomotic stricture.
Disclosures:
Jeremy Polman indicated no relevant financial relationships.
Steven Shamah: Boston Scientific – Consultant.
Jeremy Polman, DO, MS, MBA, Steven Shamah, MD. P4862 - Gastro-Jejunal Recreation and Gastro-Gastric Fistula Exclusion Using an Endoscopic Stent in a Patient With Roux-en-Y Gastric Bypass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.