St. Luke's University Health Network Bethlehem, PA
Award: ACG Presidential Poster Award
Daniel Yoon, MD1, Melkamu Adeb, MD1, Shivani Desai, MD1, Berhanu Geme, MD2 1St. Luke's University Health Network, Bethlehem, PA; 2St Luke’s University Health Network, Center Valley, PA Introduction: As cystic fibrosis (CF) survival extends into adulthood, gastroenterologists increasingly encounter gastrointestinal and hepatobiliary complications requiring new management strategies. This case introduces two treatment principles: (1) the necessity of early multimodal imaging to differentiate CF-related pathology from surgical emergencies, and (2) the importance of conservative management that avoid unnecessary interventions.
Case Description/
Methods: A 41-year-old male with CF (ΔF508 mutation), pancreatic insufficiency, and CF-related diabetes presented with progressive abdominal distension and emesis despite optimized bowel regimens. Initial CT revealed long-segment colo-colonic intussusception extending to the mid-transverse colon with moderate stool burden, complete pancreatic lipomatous pseudohypertrophy, and dilated left intrahepatic biliary tree. Follow-up MRI/MRCP demonstrated persistent intussusception, left intrahepatic biliary ductal dilation with confluence narrowing, and multiple biliary calculi. Subsequent presentation with abdominal pain and hematochezia prompted repeat imaging, showing resolution of intussusception but persistent colonic wall thickening and an enlarged appendix with hyperdense secretions. The following colonoscopy revealed distended appendix with ulcerated appendiceal orifice mucosa with purulent discharge, initially concerning for appendicitis or malignancy, though biopsy was unremarkable. Distended appendix from accumulation of thick mucinous is thought to be the pathologic lead point for colo-colonic intussusception. The patient was managed conservatively with an aggressive bowel regimen and plans for outpatient endoscopic ultrasound and ERCP, avoiding unnecessary surgical intervention. Discussion: This case illustrates essential treatment strategies for aging CF patients: early implementation of comprehensive imaging protocols (CT, MRI/MRCP, endoscopy) enables accurate differentiation of CF-related complications from acute surgical conditions, while conservative management approaches prevent unnecessary procedures. Gastroenterologists must recognize that CF-related GI pathology often mimics surgical emergencies but frequently responds to medical management and targeted endoscopic interventions. A multidisciplinary approach emphasizes careful observation, serial imaging, and selective intervention, which canimprove outcomes while minimizing procedural risks in the aging CF population.
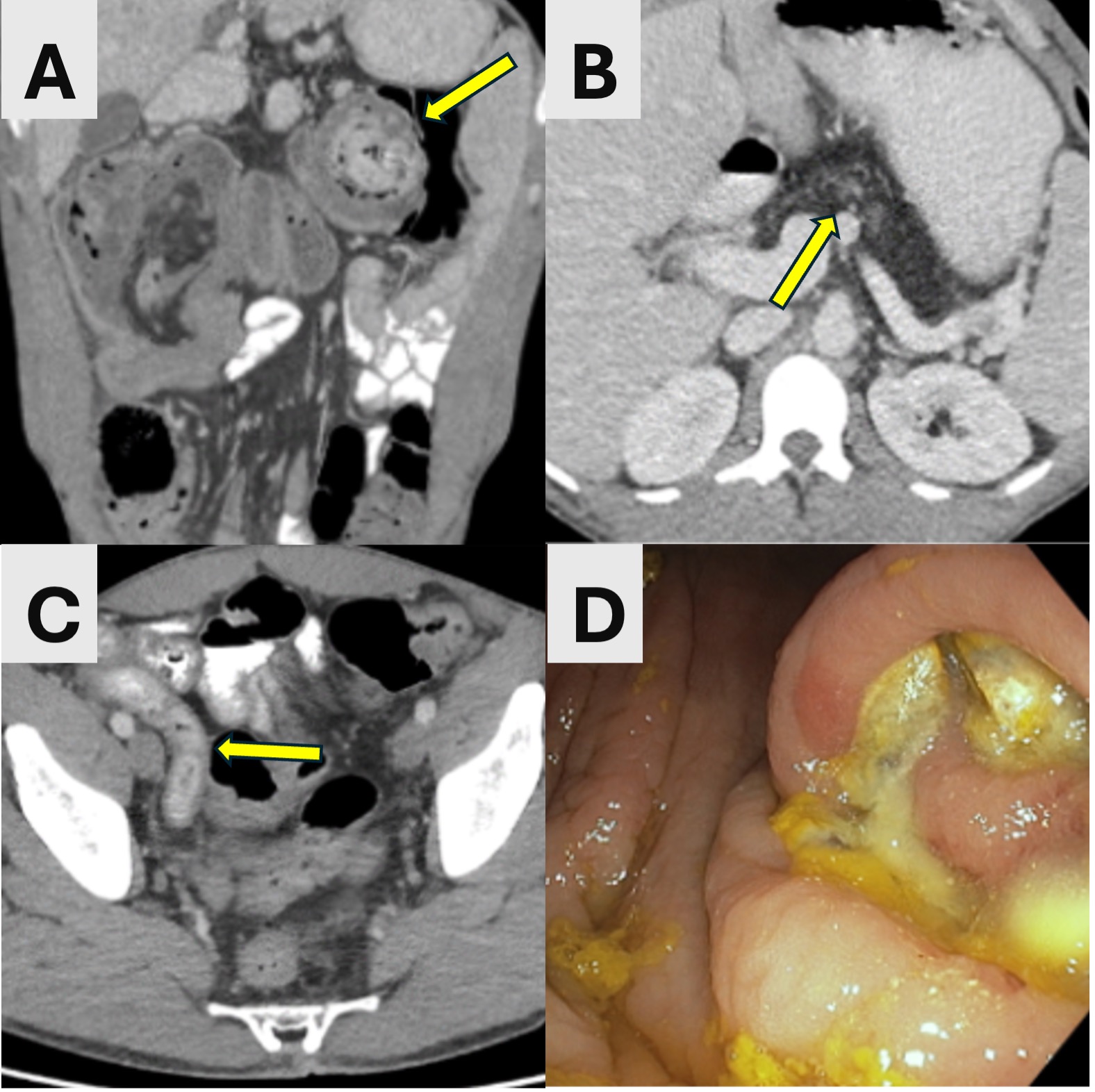
Figure: (A) Coronal image of CT abdomen demonstrates a long segment colo-colonic intussusception (arrows) with an intussusception telescoping into the intususceptum. (B) Axial CT images at the level of the upper abdomen in the same patient show complete fatty replacement (lipomatous pseudohypertrophy) of the pancreas (arrows), consistent with history of cystic fibrosis. (C) Axial CT abdomen show appendix was = noted to be markedly enlarged and sausage shape with thick intraluminal contents. (D) Colonoscopy reveal ulcerated mucosa with purulent discharge seen at the appendiceal orifice and bulge into the cecum from the appendiceal base.
Disclosures: Daniel Yoon indicated no relevant financial relationships. Melkamu Adeb indicated no relevant financial relationships. Shivani Desai indicated no relevant financial relationships. Berhanu Geme indicated no relevant financial relationships.
Daniel Yoon, MD1, Melkamu Adeb, MD1, Shivani Desai, MD1, Berhanu Geme, MD2. P4716 - Just Kidding Around: Unusual Adult Manifestation of Cystic Fibrosis With Distal Intestinal Obstruction Syndrome (DIOS), Appendiceal Disease, Biliary Pathology, and Pancreatic Manifestations, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.