Paola Pena, MD, Qusai AlMasad, MD, Hashem Ayyad, MD, MBA, Thaer Abdelfattah, MD, MPH Roger Williams Medical Center, Providence, RI Introduction: Prostate adenocarcinoma with direct rectal invasion is rare due to anatomical separation by Denonvilliers’ fascia. Patients may present with gastrointestinal symptoms, mimicking primary rectal malignancy. Early endoscopic and immunohistochemical evaluation is crucial. We present a case of prostate cancer presenting as a rectal mass with rectal bleeding, ultimately diagnosed as direct rectal invasion by prostate adenocarcinoma.
Case Description/
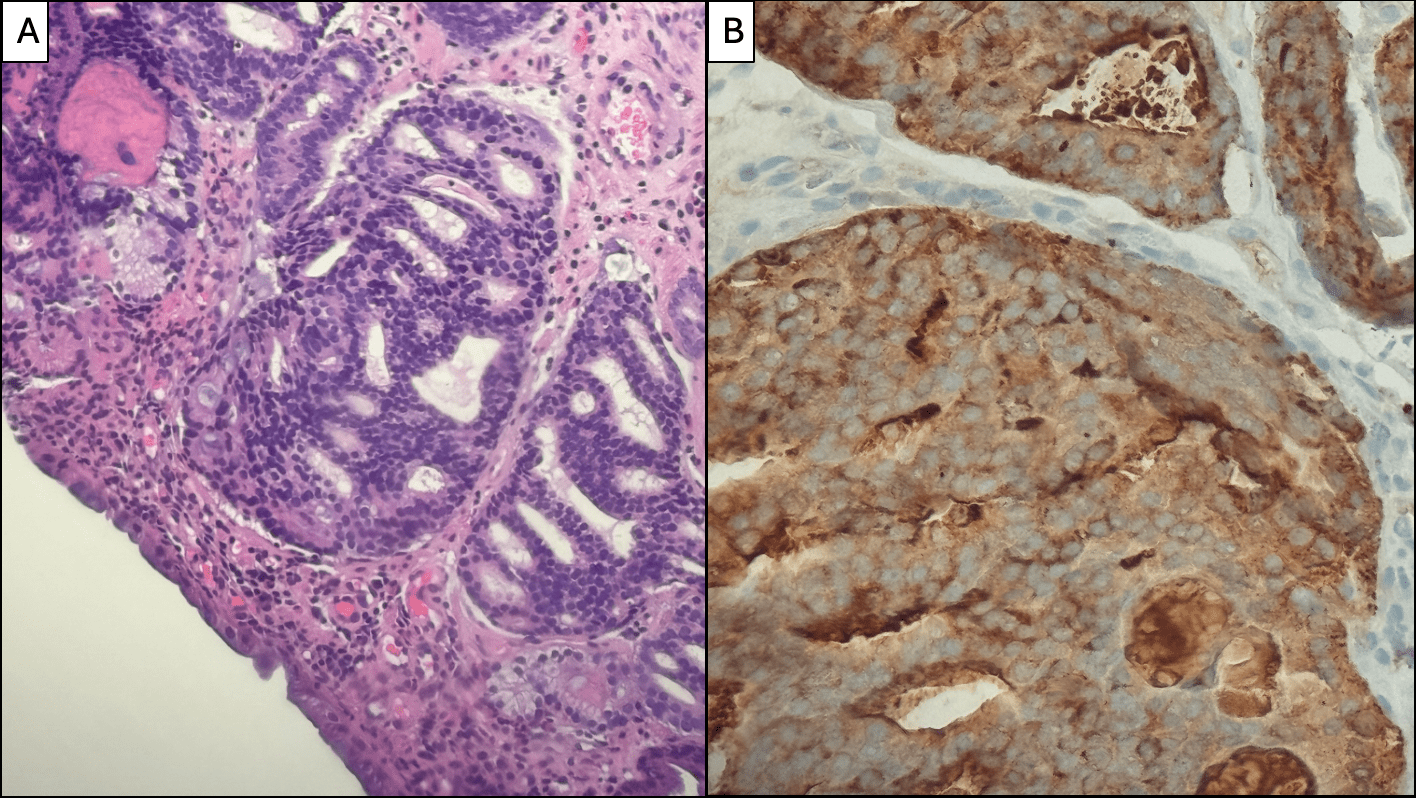
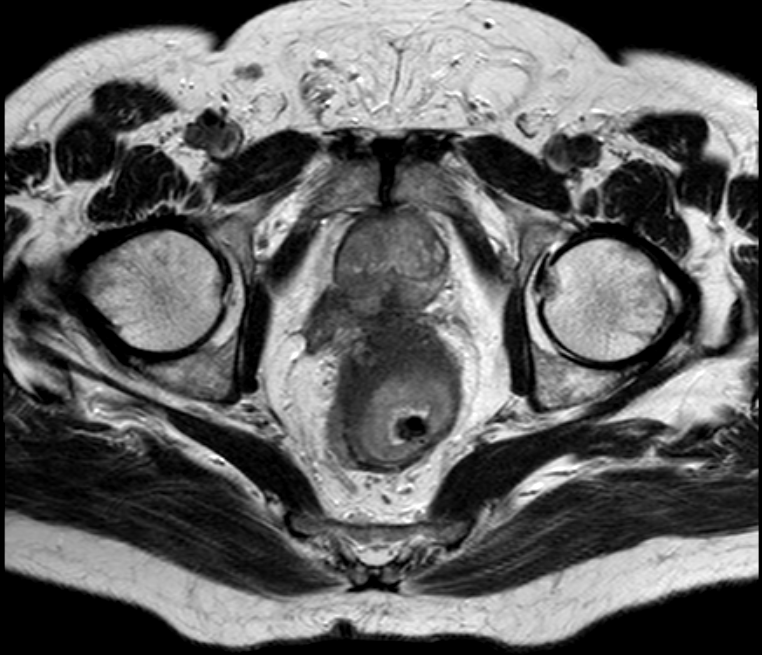
Methods: A 73-year-old male with no known past medical history was referred to gastroenterology for evaluation of rectal bleeding. He reported no bowel habit changes, pain, or weight loss. Colonoscopy revealed a large, ulcerated, non-obstructing rectal mass, partially circumferential and measuring 9 cm in length, located from 10 cm to 1 cm from the anal verge, involving approximately two-thirds of the rectal lumen. Biopsies of the lesion were obtained. Histopathology showed features consistent with prostate adenocarcinoma, supported by positive immunohistochemical staining for prostate specific antigen (PSA) and prostatic acid phosphatase (PSAP), while negative for colorectal markers (CDX2, CK20) and neuroendocrine markers. A PSMA PET scan was subsequently performed, revealing intense, heterogeneous uptake in the prostate gland, confirming the primary source of malignancy. The scan also demonstrated marked rectal wall thickening with evidence of direct rectal invasion. The patient’s serum PSA level was markedly elevated at 623.272 ng/mL. Current treatment includes both radiation therapy and hormonal therapy with lubiprostone. Discussion: This case highlights the need to consider prostate cancer with rectal invasion as a potential cause in elderly male patients presenting with rectal bleeding and rectal masses that appear atypical for primary colorectal. Although rare, direct rectal invasion can occur in advanced prostate cancer, bypassing the protective barrier of Denonvilliers’ fascia. The endoscopic appearance may mimic primary rectal cancer, and histological evaluation with PSA is key to confirming the diagnosis. Accurate identification avoids unnecessary rectal surgery and enables targeted therapy. A multidisciplinary approach is essential for effective management.
Figure: Prostate mass directly invading the rectum
Figure: A. Hematoxylin and Eosin, 400X B. Prostate specific antigen immunization (Ventana, Roche, Tucson, Arizona), 400X
Disclosures: Paola Pena indicated no relevant financial relationships. Qusai AlMasad indicated no relevant financial relationships. Hashem Ayyad indicated no relevant financial relationships. Thaer Abdelfattah indicated no relevant financial relationships.
Paola Pena, MD, Qusai AlMasad, MD, Hashem Ayyad, MD, MBA, Thaer Abdelfattah, MD, MPH. P4679 - Rectal Bleeding as the Initial Presentation of Prostate Adenocarcinoma With Direct Rectal Invasion: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.