Mount Sinai West, Icahn School of Medicine at Mount Sinai New York, NY
Alexandria Markley, MD1, Saro Aprikan, MBBCh2, Jordan Arabian, MD2, Emmanuel Rodriguez Rivera, 3, Steven Rodriguez, MD4, Frank Nelson, MD4 1Mount Sinai West, Icahn School of Medicine at Mount Sinai, New York, NY; 2Mount Sinai Morningside, Icahn School of Medicine at Mount Sinai, New York, NY; 3University of Puerto Rico School of Medicine, San Juan, Puerto Rico; 4Mount Sinai West, New York, NY Introduction: Cecal bascule is a rare form of intestinal obstruction in which the cecum folds antero-superiorly over the ascending colon, potentially leading to obstruction. The nonspecific symptoms,including abdominal pain, distention, constipation, nausea, and vomiting,make diagnosis challenging.We present a rare case of cecal bascule located just beyond the hepatic flexure.
Case Description/
Methods: A 35-year-old female with a medical history of hypothyroidismpresented with a 7-year history of chronicabdominal pain associated with bloating and constipation. Symptoms improved with defecation and worsened after eating. Physical exam was unremarkable and thyroid stimulating hormone, tissue transglutaminase, and H. pylori stool antigen were negative. She was prescribed daily Miralax for presumed irritable bowel syndrome, which initially resolved her symptoms.Three years later, she returned to theclinic with epigastric abdominal pain, bloating, and constipation despite continued daily laxative use.Colonoscopy revealed internal hemorrhoids but was aborted at the hepatic flexure due to a significantly tortuous colon. A subsequent CT colonography showed a redundant and dilated colon with a cecal bascule at the hepatic flexure. She was referred for surgical evaluation, which she deferred.She laterdeveloped worsening abdominal pain, bloating, and constipation, with significant weight loss secondary to poor oral intake. During this time, she also tested positive for small intestinal bacterial overgrowth (SIBO). Given her progressive symptoms, she optedfor right hemicolectomy, with improvement of her symptoms post-operatively. Discussion: Cecal bascule is a rare cause of obstruction, andits nonspecific symptoms oftendelay diagnosis. Unlike cecal volvulus, which presents acutely, cecal bascule may cause chronic or intermittent symptoms, as seen in our patient. She also tested positive forSIBO, likely secondary to delayed gastric transit due to functional colonic obstruction and stasis.Definitive treatment is surgical, with right hemicolectomy offering the most symptom resolution and lowest recurrence risk. Non-operative alternatives are less effective and typically reserved for high-risk patients. This case highlights the diagnostic challenges of cecal bascule, particularly in patients without classic risk factors such as prior abdominal surgery, or neurogenic bowel dysfunction and the importance of maintaining a broad differential diagnosis in patients with chronic gastrointestinal symptoms.
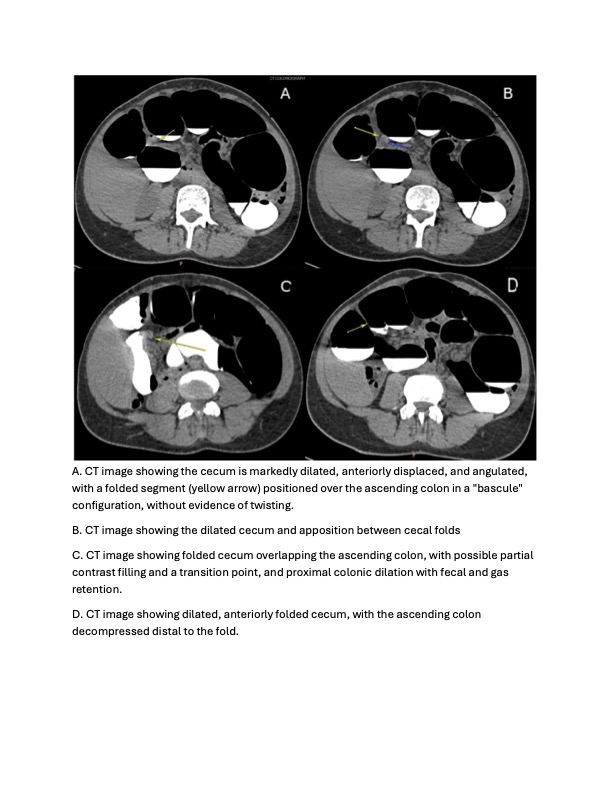
Figure: Figure 1. CT Imaging Features of Cecal Bascule
Disclosures: Alexandria Markley indicated no relevant financial relationships. Saro Aprikan indicated no relevant financial relationships. Jordan Arabian indicated no relevant financial relationships. Emmanuel Rodriguez Rivera indicated no relevant financial relationships. Steven Rodriguez indicated no relevant financial relationships. Frank Nelson indicated no relevant financial relationships.
Alexandria Markley, MD1, Saro Aprikan, MBBCh2, Jordan Arabian, MD2, Emmanuel Rodriguez Rivera, 3, Steven Rodriguez, MD4, Frank Nelson, MD4. P4635 - When Common Symptoms Conceal a Rare Diagnosis: A Case of Cecal Bascule, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.