Nishtar Medical University and Hospital Multan, Punjab, Pakistan
Ali Mehdi, MBBS1, Syed Mohsin Raza Bukhari, MBBS1, Hassan Mehdi, MBBS1, Hafiz Ahmad, 1, Maham Zaman, MBBS2, Aqsa Farooq, MBBS1, Amna Zaheer, 3, Shahan Javed, 4 1Nishtar Medical University and Hospital, Multan, Punjab, Pakistan; 2Quaid-e-Azam Medical College, Bahawalpur, Punjab, Pakistan; 3Liaquat National Hospital and Medical College, Karachi, Sindh, Pakistan; 4Alfaisal University, Riyadh, Ar Riyad, Saudi Arabia Introduction: Chilaiditi’s sign, a rare radiological finding described more than a century ago by Demetrious Chilaiditi, is characterized by the interposition of the colon between the liver and diaphragm. It is known as Chilaiditi syndrome when associated clinical symptoms manifest. This condition may have a spectrum of symptoms, rarely involving the cardiac system. Radiological imaging remains the cornerstone of diagnosis. It is usually managed conservatively, but surgical intervention may be required in some cases.
Case Description/
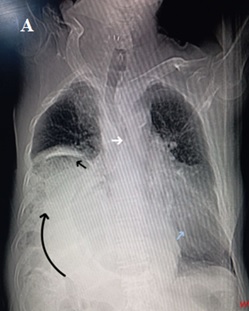
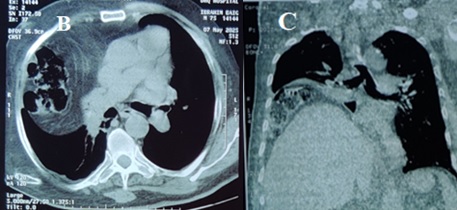
Methods: A 75-year-old male with a 10-year history of COPD presented with complaints of fever, dyspnea, productive cough, chest pain, and abdominal discomfort for the past 3 days. Associated symptoms included burning chest sensation, bloating, and constipation for a week. He had been a heavy smoker for 45 years and an alcoholic for 30 years. A chest X-ray chest revealed air under the right hemidiaphragm (Figure 1-A). HRCT was obtained showing marked superior displacement of the right hemidiaphragm with superior displacement of abdominal contents (Liver and Ascending colon) into the thoracic cavity causing contralateral displacement of mediastinum. Gut loops were lying between the diaphragm and liver, in keeping with Chilaiditi syndrome (Figure 1-B, C). He was managed conservatively and discharged upon the resolution of symptoms. Discussion: Chilaiditi syndrome, having a worldwide incidence of 0.25% to 0.28%, arises due to pathology or anatomical variation in suspensory ligaments of the colon. Gastrointestinal symptoms including abdominal pain, vomiting, nausea, and constipation are common, with cardiorespiratory symptoms being less frequent. It is often misdiagnosed as bowel perforation or pneumoperitoneum. Ascites, obesity, and chronic obstructive lung disease are among its risk factors. Our case aims to highlight the diagnostic challenge of recognizing Chilaiditi syndrome in patients with coexisting abdominal and cardiorespiratory symptoms and to emphasize its consideration in the differentials of a COPD patient having abdominal symptoms. X-ray and CT scan remain crucial to identify this condition. It is a benign condition that can be managed conservatively but may lead to severe complications including bowel obstruction, perforation, and volvulus of the cecum which may require surgical intervention.
Figure: Figure 1. Figure A: Chest X-ray showing air under the right hemidiaphragm (dilated gut loops of the ascending colon), mediastinal shifting, and consolidation in the left lung.
Figure: Figure B, C: HRCT showing gut loops of ascending colon in the mediastinum, liver above the level of contralateral diaphragm, and gut loops between right hemidiaphragm and the liver.
Disclosures: Ali Mehdi indicated no relevant financial relationships. Syed Mohsin Raza Bukhari indicated no relevant financial relationships. Hassan Mehdi indicated no relevant financial relationships. Hafiz Ahmad indicated no relevant financial relationships. Maham Zaman indicated no relevant financial relationships. Aqsa Farooq indicated no relevant financial relationships. Amna Zaheer indicated no relevant financial relationships. Shahan Javed indicated no relevant financial relationships.
Ali Mehdi, MBBS1, Syed Mohsin Raza Bukhari, MBBS 1, Hassan Mehdi, MBBS1, Hafiz Ahmad, 1, Maham Zaman, MBBS2, Aqsa Farooq, MBBS1, Amna Zaheer, 3, Shahan Javed,4. P4632 - Chilaiditi Syndrome in a Patient with COPD: A Rare Entity, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.