University of New Mexico Health Sciences Center Albuquerque, NM
Moon Ryu, MD1, Udita Gupta, MD1, Euriko Torrazza Perez, MD, MSPH2 1University of New Mexico Health Sciences Center, Albuquerque, NM; 2University of New Mexico, Albuquerque, NM Introduction: Hepatocellular carcinoma (HCC) is the most common primary liver malignancy, often associated with underlying cirrhosis. While HCC typically remains confined to the liver, it can invade adjacent structures. Gastric involvement by HCC is rare and may occur through direct invasion or metastatic spread. This case underscores the importance of considering gastric invasion in patients with large HCCs presenting with gastrointestinal symptoms.
Case Description/
Methods: A 67-year-old male with history of HCV complicated by cirrhosis treated in 2016 with ledipasvir/sofosbuvir presented with progressively worsening nausea and abdominal pain for two weeks.
He initially presented to another hospital two weeks prior with complaints of abdominal pain and nausea for three days. A CT Abdomen/Pelvis with contrast found a heterogenous mass in the left lobe of the liver measuring approximately 10 x 8.7 x 9.3cm. He was discharged from the ED with plan for outpatient follow-up.
In these last two weeks, he reported his epigastric abdominal pain had become severe and he had significant nausea resulting in poor PO intake and a 10lb weight loss. He also noticed a growing visible prominent mass in his epigastrium.
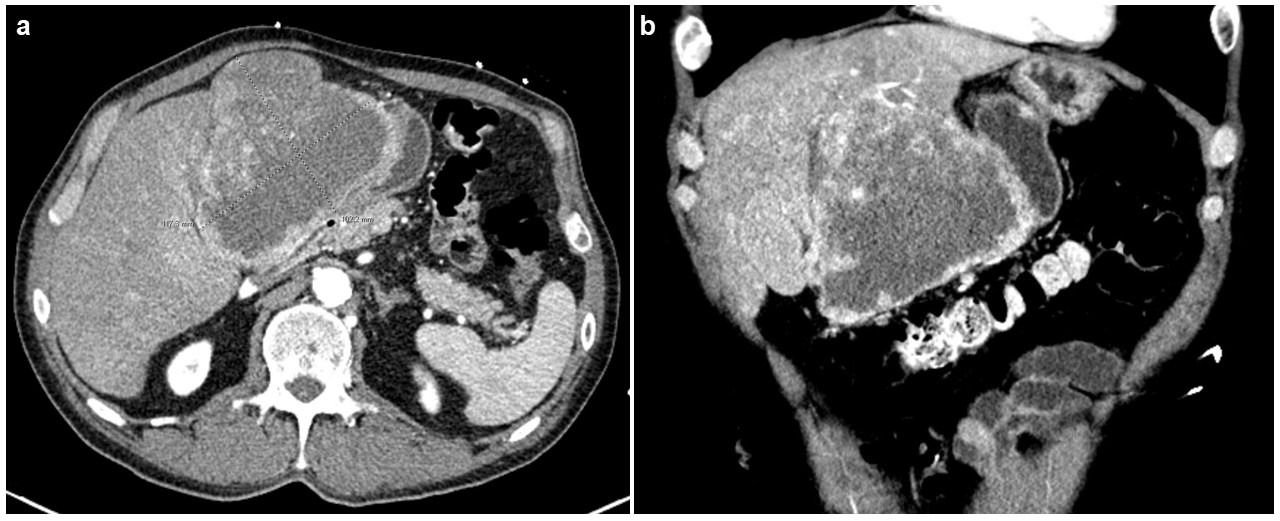
On admission, his vital signs were within normal limits. On physical exam, a severely tender, visible RUQ abdominal mass extending to the midline was noted. Pertinent lab findings included AFP of 9624, platelets of 547, albumin of 3.5, AST of 125, ALT of 31, Alk. Phos. of 239, INR of 1.30, and an undetectable HCV RNA PCR. The 3-phase CT of the liver found findings of cirrhosis with a large lesion replacing the left lobe measuring 10.2 x 11.8cm and compression on the distal body of the stomach.
Hepatobiliary surgery was consulted with tentative plan made for left hepatectomy. Prior to the operation, the patient had a cardiac arrest with emergent intubation complicated by “feculent material in the airway”. Following multiple rounds of CPR and continued PEA rhythm, resuscitation efforts were discontinued after discussion with the patient’s family. Discussion: The above case demonstrates a patient with large HCC with rapid growth and probable gastric invasion. The feculent appearing material was likely necrotic tumor contents that eroded into the stomach resulting in aspiration and the patient’s death. Recent evidence has supported surgical resection as a possible next step and expedited management may be prudent to avoid complications of invasion from aggressive lesions.
Figure: Triple phase CT Abdomen/Pelvis showing the large liver lesion in (a) axial and (b) coronal views.
Disclosures: Moon Ryu indicated no relevant financial relationships. Udita Gupta indicated no relevant financial relationships. Euriko Torrazza Perez indicated no relevant financial relationships.
Moon Ryu, MD1, Udita Gupta, MD1, Euriko Torrazza Perez, MD, MSPH2. P5980 - Hepatocellular Carcinoma With Suspected Gastric Involvement, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.