University of Texas Health Sciences Center in Houston Houston, TX
Nina Quirk, MD, MS1, Maneera T. Chopra, MD2, Kazi Haque, MD3 1University of Texas Health Sciences Center in Houston, Houston, TX; 2McGovern Medical School at UTHealth Houston, Houston, TX; 3University of Texas Health Science Center, Houston, TX Introduction: Hepatic actinomycosis is a rare bacterial infection caused by Actinomyces, often misdiagnosed due to its indolent course and nonspecific presentation. IgG4-related disease (IgG4-RD) is a fibroinflammatory condition that can affect the hepatobiliary system usually resulting in cholestasis, jaundice, and rarely, liver masses. We present a unique case of hepatic actinomycosis initially suspected as IgG4-RD.
Case Description/
Methods: A 71-year-old man presented in August 2024 with abdominal pain, night sweats, and 40-pound weight loss. Prior CT abdomen in February 2024 revealed a 10 cm liver mass. Liver biopsy showed prominent inflammatory infiltrate. He was admitted at our institution in June 2024 for similar complaints. CT abdomen revealed large right hepatic hypodense mass with scattered small right hepatic hypodense lesions. Entamoeba, echinococcus, histoplasma, leishmania antibodies, AFP, CA 19-9, CEA, C3/4, ANA, syphilis were all unremarkable. Liver biopsy in June 2024 showed abundant mixed inflammatory cells and associated fibrosis. Spirochete, fungal, and acid-fast bacilli stains were negative. IgG and IgG4 immunostains showed a ratio of IgG4:IgG greater than 40% and IgG4 positive plasma cells were greater than 100/HPF. During admission in August 2024 for continued fever, chills and failure to thrive, CT abdomen showed findings similar to prior. MRI liver just two days later revealed interval new rim enhancing lesions. IgG level was 3,220 mg/dL (649 mg/dL subclass 4). Rheumatology was consulted for IgG4-RD and remarked that this would be a very unusual presentation of IgG4-RD. The patient continued to have fever and little clinical improvement despite being on piperacillin/tazobactam. Liver biopsy in August 2024 showed mixed inflammation, IgG4:IgG more than 30%, IgG4 positive plasma cells greater than 50/HPF and, after meticulous review, sulfur granules. Sulfur granules are suggestive of Actinomyces infection. Rheumatology advised against immunosuppression given low likelihood of IgG4-RD. The patient was started on treatment for actinomycosis with augmentin. Outpatient CT abdomen in December 2024 showed interval improvement of abscesses with no rim enhancement. Discussion: This is a rare case of hepatic actinomycosis mimicking IgG4-related hepatobiliary disease. Actinomyces infection may induce an immune response that leads to elevated IgG4 levels. This case contributes to the limited number of available case reports on hepatic actinomycosis and highlights potential diagnostic pitfalls.
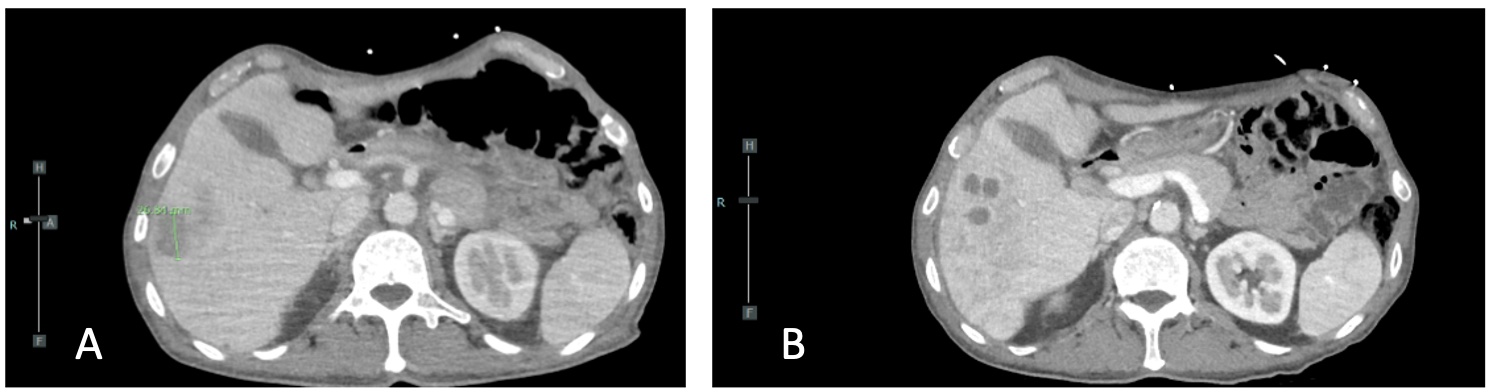
Figure: Image A: CT abdomen/pelvis June 2024 showing liver mass. Image B: CT abdomen/pelvis August 2024 showing progressing hypodense lesions.
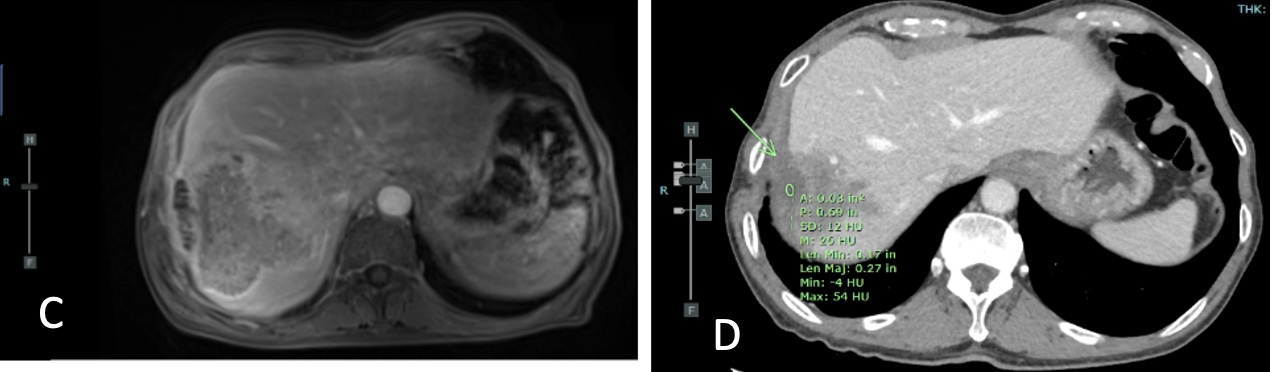
Figure: Image C: MRI liver protocol showing interval growth of liver mass with rim enhancement. Image D: CT abdomen/pelvis December 2024 showing improvement in size if liver mass with no rim enhancement.
Disclosures: Nina Quirk indicated no relevant financial relationships. Maneera Chopra indicated no relevant financial relationships. Kazi Haque indicated no relevant financial relationships.
Nina Quirk, MD, MS1, Maneera T. Chopra, MD2, Kazi Haque, MD3. P6146 - Mistaken Identity: A Rare Case of Hepatic Actinomycosis Initially Suspected as IgG4-Related Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.