University of Iowa Hospitals & Clinics Coralville, IA
Tewodros T. Ayele, MD, MPH University of Iowa Hospitals & Clinics, Coralville, IA Introduction: A 68-year-old man with multiple comorbidities, including recent VP shunt placement, was found to have a 6.5 cm proximal jejunal mass on CT performed for elevated WBC. Push enteroscopy revealed a 5 cm fungating lesion; biopsy confirmed intestinal-type adenocarcinoma with mucinous features. MMR testing showed loss of MSH6 and diminished MSH2, highly suggestive of Lynch syndrome. He underwent en bloc surgical resection and was referred for genetic counseling and germline testing.
Case Description/
Methods: A 68-year-old male with a history of NPH (VP shunt a month prior to presentation), CAD, GERD, chronic iron deficiency anemia, prostate cancer (post-radiotherapy), left carotid stenosis causing CVA status post endarterectomy, was transferred for evaluation of a proximal jejunal mass. The mass was incidentally discovered during imaging performed for elevated WBC post-VP shunt, raising concern for infection. CT abdomen/pelvis showed a 6.5 × 5.1 × 6.3 cm aneurysmal dilatation with heterogeneous enhancement in the proximal jejunum beyond the ligament of Treitz, suspicious for malignancy. Concern for microperforation led to empiric antibiotics prior to transfer.
The patient had chronic iron deficiency anemia with normal EGD and colonoscopy in Nov 2024. He had a 40 pack-year smoking history (recently quit) and a family history of colon cancer (father at age 75) and lymphoma (mother).
Labs showed WBC 12.2 (down from 21), Hgb 7.5, platelets 333, and iron studies consistent with iron deficiency anemia. CMP was unremarkable.
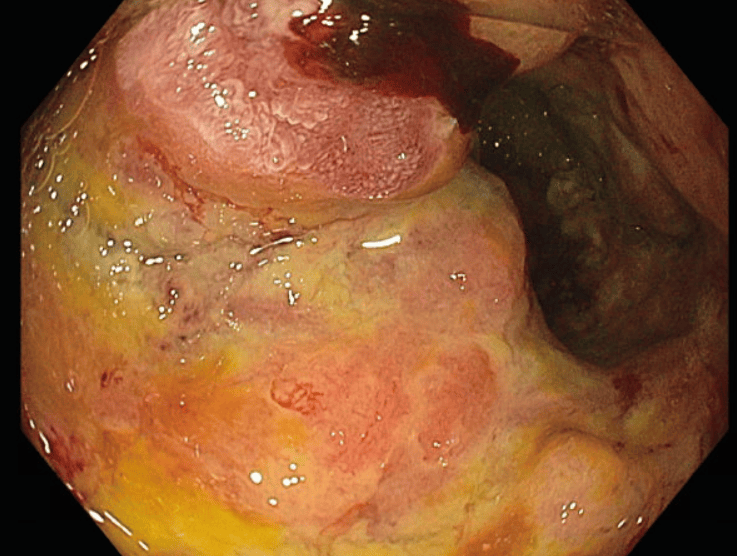
Push enteroscopy revealed a 5 cm eroded, fungating, apple-core lesion from D3–D4 into proximal jejunum. Biopsies confirmed adenocarcinoma, an intestinal type with mucinous features. MMR IHC showed MSH6 loss and markedly diminished MSH2, with intact MLH1 and PMS2, highly suggestive of Lynch syndrome.
The patient underwent en bloc resection (proximal jejunum, D3/D4, partial colectomy, cholecystectomy). Postoperative recovery was uneventful. He was referred to cancer genetics for germline testing. Discussion: This case highlights a rare presentation of Lynch syndrome as proximal jejunal adenocarcinoma. Small bowel tumors are uncommon and may be the first or only sign of Lynch syndrome. In this patient, abnormal leukocyte count led to imaging and enteroscopy, revealing a mucinous adenocarcinoma. MMR IHC showed loss of MSH6 and diminished MSH2, suggesting Lynch syndrome. Recognition of abnormal MMR is key for diagnosis, guiding genetic testing, and identifying at-risk family members.
Figure: Enteroscopy image of apple core lesion
Figure: CT showing mass in the proximal Jejunum
Disclosures: Tewodros Ayele indicated no relevant financial relationships.
Tewodros T. Ayele, MD, MPH. P6226 - First Presentation of Lynch Syndrome as Incidentally Found Duodenojejunal Adenocarcinoma in a 68-Year-Old Male, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.