Tuesday Poster Session
Category: Stomach and Spleen
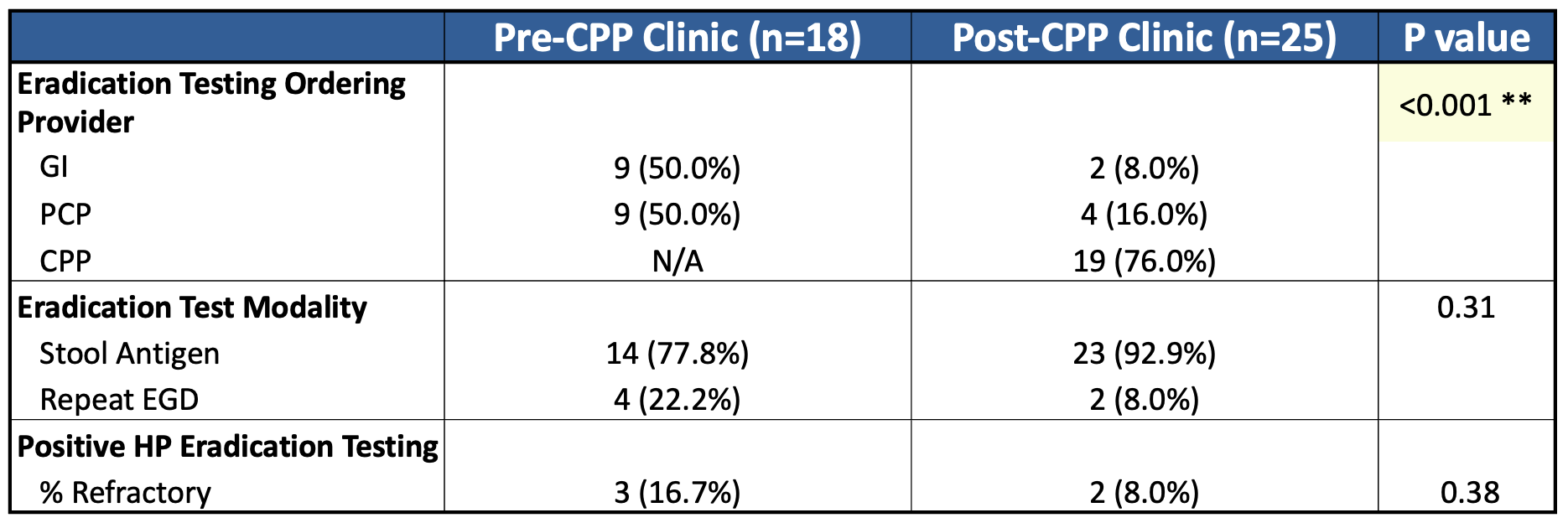
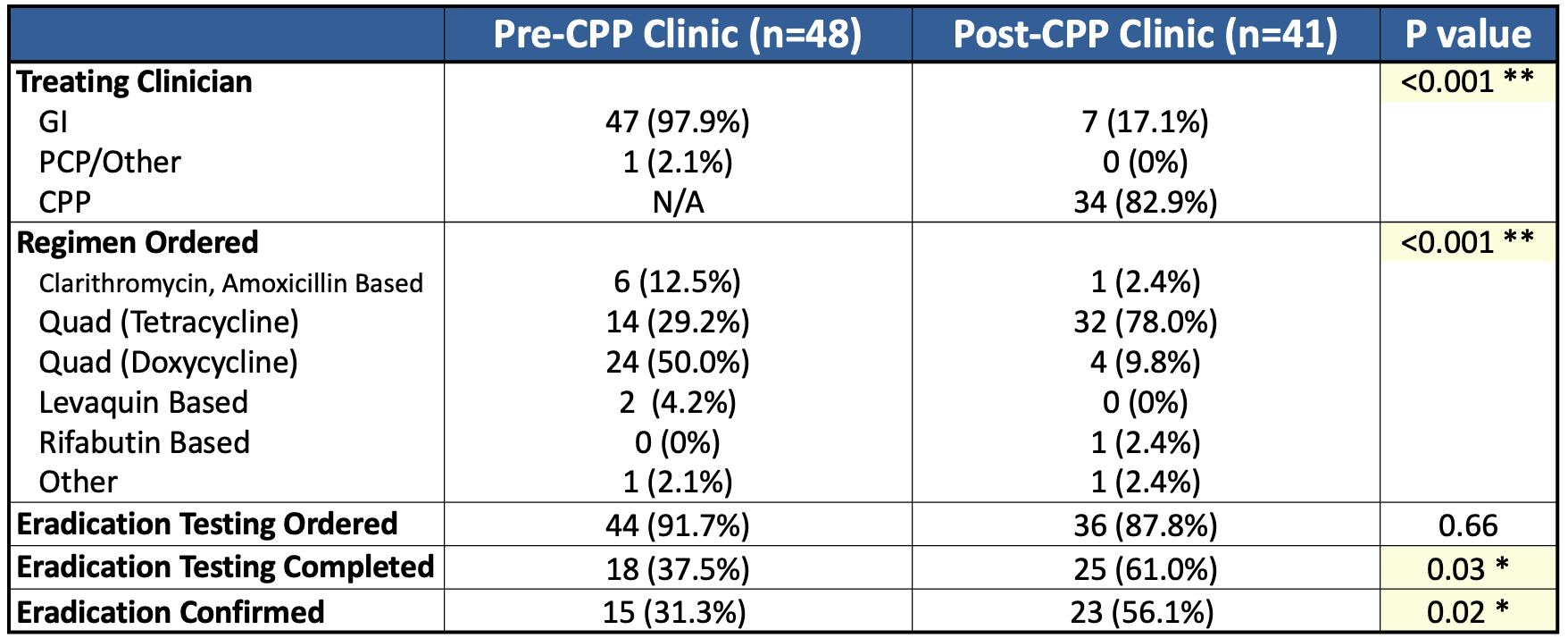
Improving <i>Helicobacter pylori</i> Eradication Testing Rates Through a Dedicated Pharmacy Clinic: A Quality Improvement Initiative


.jpg "Samantha A. Menegas, MD photo")
Samantha A. Menegas, MD
Duke University Hospital
Durham, NC