Mina Awadallah, MD, MSc1, Nakul Bhardwaj, DO, MPH1, John Erikson Yap, MD, MBA, FACG2 1University of Utah, Salt Lake City, UT; 2University of Utah Health, Salt Lake City, UT Introduction: Right upper quadrant (RUQ) pain following meals is a common clinical presentation often attributed to hepatobiliary pathology, peptic disease, or functional gastrointestinal disorders. Congenital anomalies of the duodenum, particularly duplication of the duodenal lumen, are exceedingly rare in adults and seldom considered in the differential. We present a unique case of chronic postprandial RUQ pain associated with a congenital duodenal septum.
Case Description/
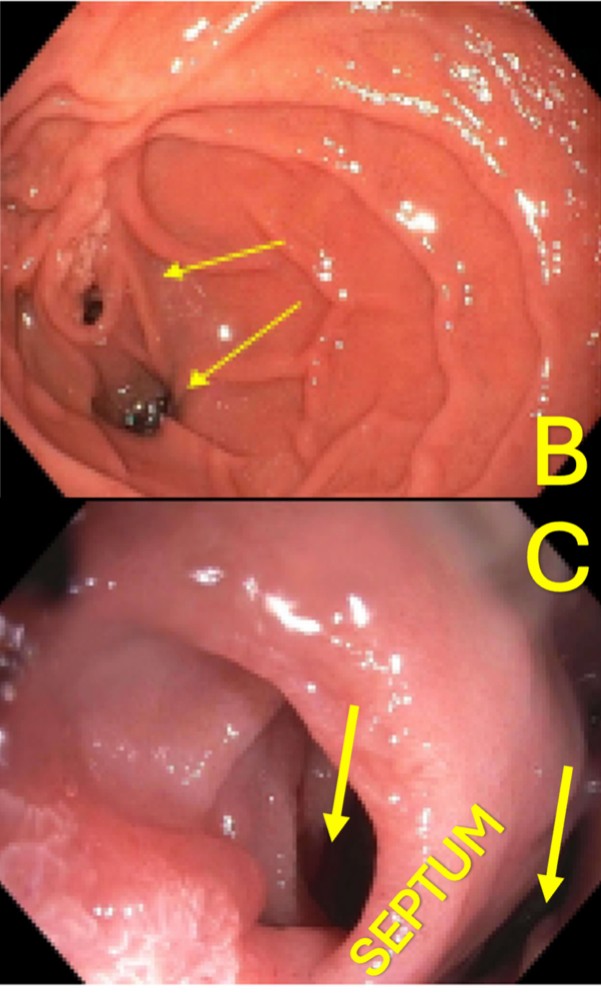
Methods: A 44-year-old woman with a history of thyroid disease, anxiety, and hyperlipidemia, and no prior abdominal surgeries, was referred for evaluation of chronic right upper quadrant (RUQ) pain. She described a pressure-like discomfort and bloating occurring 1–2 hours after meals, localized to the RUQ. She reported a sensation that food feels "stuck" in that area, with symptoms persisting for several hours before resolving spontaneously. Initial laboratory evaluation, including complete blood count (CBC) and comprehensive metabolic panel (CMP), was within normal limits. A CT abdomen was initially read as unremarkable. However, upper endoscopy revealed a mildly dilated second portion of the duodenum with two lumens that communicated distally at the third portion of the duodenum (Images B & C). Endoscopic biopsies were unremarkable. Following endoscopic findings, the CT abdomen was re-reviewed in collaboration with radiology, revealing a congenital duodenal septum at the second portion of the duodenum (Image A). Given the correlation between symptoms and oral intake, along with the localized duodenal anomaly, it is likely that transient food retention in the septated segment contributes to her postprandial discomfort. Discussion: This case highlights a rare duodenal congenital anomaly as a cause of postprandial RUQ pain. While such septa are typically diagnosed in pediatric populations, incidental findings in adults are possible. Multidisciplinary discussion is underway to evaluate the utility of surgical or endoscopic septotomy. Recognition of such rare congenital findings can alter clinical management and highlights the importance of thorough endoscopic and radiologic evaluation in patients with unexplained gastrointestinal symptoms.
Figure: A. CT Imaging showing congenital septum in the duodenum.
Figure: B & C. Endoscopic image of the 2nd portion of the duodenum (yellow arrows pointing to the lumen).
Disclosures: Mina Awadallah indicated no relevant financial relationships. Nakul Bhardwaj indicated no relevant financial relationships. John Erikson Yap: Phathom Pharmaceutical – Speakers Bureau. Steris – Consultant.
Mina Awadallah, MD, MSc1, Nakul Bhardwaj, DO, MPH1, John Erikson Yap, MD, MBA, FACG2. P6299 - Unraveling a Congenital Duodenal Septum: A Rare Cause of Postprandial RUQ Pain in an Adult Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.