Samar Pal S. Sandhu, MBBS, Nakul Mahajan, MBBS, Kantash Kumar, MBBS, Neha Sharma, MD, Yasutoshi Shiratori, MD Maimonides Medical Center, Brooklyn, NY Introduction: Diffuse gastric adenocarcinoma (DGA) is a less common type of gastric cancer and often presents at an advanced stage due to minimal mucosal changes, submucosal infiltrative growth, and false-negative reports on superficial endoscopic biopsies. We present a case of advanced DGA presenting with gastric outlet obstruction (GOO) initially mischaracterized as CMV gastritis due to confounding endoscopic and histopathologic findings.
Case Description/
Methods: A 50-year-old man with a history of flaccid paraplegia due to a motor vehicle accident underwent esophagogastroduodenoscopy (EGD) for complaints of 2 months of intermittent nausea, vomiting, dysphagia, and constipation, raising concerns for GOO. EGD revealed an antral ulcerated mass with significant thickening, with histology showing reactive gastropathy and chronic gastritis with atypia, but no carcinoma. He was started on PPI therapy, and a repeat EGD in 4 weeks showed a persistent ulcer positive for CMV on IHC, resulting in initiation of IV ganciclovir. Given no relief of symptoms, the patient presented to the ED. Inpatient EGD revealed severe circumferential ulceration, friable mucosa, and significant pyloric narrowing. Endoscopic ultrasound (EUS) indicated invasion into the muscularis propria but without serosal involvement.
Histology was consistent with high-grade DGA with poorly cohesive cells. Molecular analysis was negative for HER2 and showed retained DNA repair abnormalities. Serum CMV PCR and tissue CMV immunohistochemistry were negative with no viral inclusions.
The patient underwent laparoscopic distal gastrectomy with Roux-en-Y gastrojejunostomy for malignant GOO, with intraoperative findings including peritoneal implants. Histology revealed invasion through the gastric wall to the serosal surface with metastatic spread involving lymphovascular, perineural, hepatogastric, and omental margins, confirming advanced disease. Discussion: DGA has an increased incidence in the younger population and is associated with high morbidity and mortality due to advanced stage at presentation. Studies have shown CMV to have high prevalence in gastric cancer tissue with unclear clinical significance. Clinicians should be vigilant, as it can lead to inaccurate diagnosis and management. Our case emphasizes the limitations of superficial biopsies, the need for adequate sampling by using techniques such as tunnel biopsies or EUS-guided sampling to improve diagnostic yield in high-suspicion cases for accurate diagnosis of DGA.
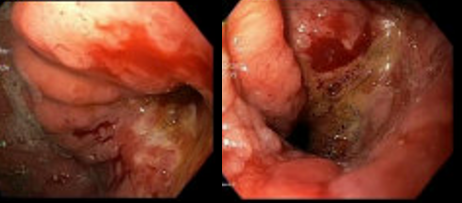
Figure: EGD showing circumferential ulceration, friable mucosa, and significant narrowing at the pylorus.
Figure: EUS showing invasion into the muscularis propria but without serosal involvement.
Disclosures: Samar Pal Sandhu indicated no relevant financial relationships. Nakul Mahajan indicated no relevant financial relationships. Kantash Kumar indicated no relevant financial relationships. Neha Sharma indicated no relevant financial relationships. Yasutoshi Shiratori indicated no relevant financial relationships.
Samar Pal S. Sandhu, MBBS, Nakul Mahajan, MBBS, Kantash Kumar, MBBS, Neha Sharma, MD, Yasutoshi Shiratori, MD. P6376 - Diffuse-Type Gastric Adenocarcinoma Masked by Cytomegalovirus Gastritis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.